
NASOGASTRIC TUBE INSERTION
REQUIREMENTS:
Verbal consent, Gloves, Fine bore nasogastric tube (feeding only) or nasogastric “Ryles” tube 16Fr (all other indications), lubricant, Syringe, Securing device (sticking), Cup of water (may be required)
PROCEDURE:
Ask the patient to breathe in through each nostril separately to judge which is more patent.
For this procedure the patient should be positioned on the bed upright and facing forward (sniffing position). Put on your gloves.
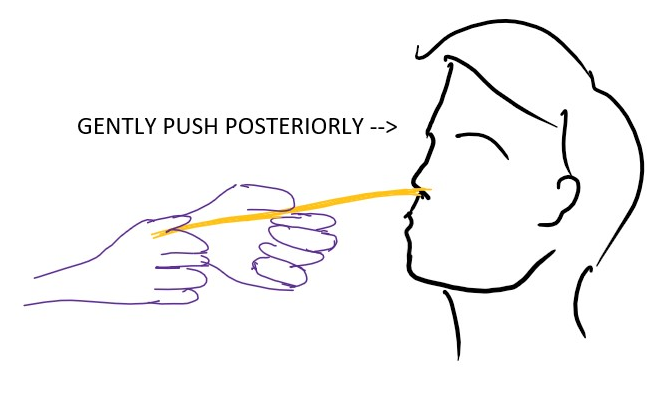
Lubricate the tip of the tube and begin to insert through one of the nostrils keeping the tube posteriorly parallel to the floor of the nose. If any resistance is encountered change to the other nostril.
Once nasopharynx is reached, ask the patient to flex their head and swallow water/ saliva.
As they swallow advance the tube to the desired length.
At the end of the procedure, air filled syringe is attached and air is pushed in while auscultating at the epigastrium.
A swoosh/ pop sound confirms the location of tube in the stomach.
Fix the tube in place using sticking.

- NOTE:
If the tube enters larynx the patient may gag or cough. Pause for a moment, withdraw slightly, ease the patient and then continue inserting it again.
For patients in supine position, slightly flex their neck while inserting the tube.
For unconscious patients, intubation in lateral decubitus has a higher success rate according to a pubmed article (https://pubmed.ncbi.nlm.nih.gov/28544238/).
PRACTICAL TIPS AND TRICKS:
1) A gentle curve can be created in the Ryle’s tube by winding it around our finger before insertion. Then while inserting the tube, let that slight curve point down.
VIDEO LINK:
Hey....the position is usually said to be flexed neck and not sniffing dog
ReplyDelete2) Add smtg abt ngt insertion in bedridden patients lets say a cva case or a comatose patient who wont be able to sit
3) you can make a column below every procedure called "also read" and mention few theoritical topics or points which one can read ..like for this one it can be ..how to measure d length ..color coding and sizes of ngt..other ways of conforming the position....meaning of different marks on the tube
3) I dont agree with the "curve ihe tube little bit part" bcz trachea is anterior to oesophagus ..if we curve there r more chances of it gng into trachea..
Thanks