Quiz question: ST elevation in aVR and ST depression in other leads is suggestive of?

Thursday, August 2, 2018
Sunday, July 29, 2018
Trapezius and pericarditis.
Suppose a patient of 40 years of age male comes to you with complaints of chest pain which is often heavy, squeezing and crushing.
You make up the diagnosis of MI based upon the symptoms in your mind. Proceeding for proper history of case you ask patient if the pain is radiating type.
Patient explains you that the pain is radiating and he is eventually experiencing pain in to the back of this some muscle. You find out that he is pointing towards the "Trapezius muscle" .
Patient explains you that the pain is radiating and he is eventually experiencing pain in to the back of this some muscle. You find out that he is pointing towards the "Trapezius muscle" .
Now, this should raise an alarm in your mind. You should stop thinking about MI.
Reason?
Both NSTEMI and STEMI shows pain which is radiating in nature. Pain involves the central portion of the chest, sometimes epigastrium and occasionally it radiates to the arms. Less common involves back, neck, lower jaw. Pain can radiate as high as occipital area but never below umbilicus.
but it never radiates to trapezius.
but it never radiates to trapezius.
Depicting exact lines of Harrison textbook of medicine.
"Radiation of discomfort to the trapezius is not seen in patients with STEMI and is useful in correct diagnosis of pericarditis"
Now, why pain radiates to trapezius?
Pericarditis, as name suggests inflames the pericardial sac of the heart. This causes irritation of the vagus nerve supplying heart. Vagus nerve is affected because it is closely related to pericardial sac. Vagus nerve acts as the afferent nerve fibers. These fibers reaches nucleus tractus solitarius in the medulla oblongata. From there it comes downwards reaches cervical plexus C2, C3 and C4. From there, the nerve fibers formed supplies lower part of trapezius.
Trapezius nerve supply:
Upper part is supplied by the spinal accessory nerve.
Lower part is supplied by the nerves from C3 and C4 only.
Upper part is supplied by the spinal accessory nerve.
Lower part is supplied by the nerves from C3 and C4 only.
Hence pain radiates to trapezius in pericarditis.
-Vipul and Ojas.
Update from IkaN: It's wrong to say that the pain of MI "never" radiates to the trapezius (which is in the back) because occasionally, pain of MI can radiate to the back. Also, pain radiating to the back should alarm you to a more serious diagnosis - aortic dissection.
Wednesday, July 18, 2018
Can you find Asterixis in Non-Hepatic disorders?
Hello Awesomites! :D
This doubt came to my mind when I saw a case of COPD with
asterixis.
"Asterixis"is a non-specific sign. It is also
known as flapping tremor.
It is a non-specific neurologic finding which may accompany
organic delirium in a variety of metabolic or toxic disorders which interfere
with cerebral metabolism.
It can be found in the cases with:-
1. Chronic pulmonary insufficiency
2. Uremia
3. Drug induced electrolyte imbalance
4. Arterial hypoxemia
5. Other reasons of electrolyte imbalance.
Upasana Y. :)
Thursday, July 12, 2018
Authors' diary: Ponder
We were discussing a case today and learnt how important it is to take a second to think before we do something when dealing with patients.
Before you get a CT scan on the patient in the ER, stop and think - does the patient really need a CT scan? Will it get me the answers I'm looking for? Or will I need additional testing? Think of the harms of radiation exposure. Unless you don't want to rule out a hemorrhage that requires immediate intervention, do not order it STAT.
Before you get a CT scan on the patient in the ER, stop and think - does the patient really need a CT scan? Will it get me the answers I'm looking for? Or will I need additional testing? Think of the harms of radiation exposure. Unless you don't want to rule out a hemorrhage that requires immediate intervention, do not order it STAT.
Tuesday, July 3, 2018
Dentinoenamel Junction
- DEJ appears as a scalloped line.
- The convexities of scallop are directed towards the dentine
- The surface of dentine appears pitted
- DEJ provides strength to the union between enamel and dentin
Clinical Significance:
- Prevents shearing of enamel when functioning.
- Scalloping of the junction is seen more in the occlusal portion where masticatory stresses are high.
- Written by Anisha Valli
Enamel Lamellae
Thin, leaf-like structure that extends from enamel surface towards DEJ
Sometimes, they penetrate towards DEJ
They consist of organic material but with a little amount of mineral content.
Types of enamel lamellae:
Type A is restricted to enamel
Type B and C are restricted to dentine
Clinical Significance:
Sometimes, they penetrate towards DEJ
They consist of organic material but with a little amount of mineral content.
Types of enamel lamellae:
- Type A: Lamelle composed of poorly calcified rod segments
- Type B: Lamelle consists of degenerated cells
- Type C: Lamelle arising in erupted teeth where cracks are filled with organic material, originating from saliva
Type A is restricted to enamel
Type B and C are restricted to dentine
Clinical Significance:
- It is a site of weakness in a tooth.
- It forms a road of entry for bacteria to initiate caries.
Written By Anisha Valli
Hunter-Schrengar bands
The change in the direction of rods is responsible for Hunter Schregar bands.
These bands are the functional adaptation to occlusal masticatory forces.
Alternating, light and dark bands of varying width that can be seen in longitudinal cross-section under the obliquely reflected light.
Dark bands: Parazones
Light Bands: Diazones
The angle between the bands is 40 degrees
- Written by Anisha Valli
These bands are the functional adaptation to occlusal masticatory forces.
Alternating, light and dark bands of varying width that can be seen in longitudinal cross-section under the obliquely reflected light.
Dark bands: Parazones
Light Bands: Diazones
The angle between the bands is 40 degrees
- Written by Anisha Valli
Zone Of Weil
Zone of Weil is present below the odontoblastic zone.
- Its a layer of 40um.
- It is also known as the sub-odontoblastic layer.
- It doesn't consist of cells.
- This zone is prominently seen in the coronal pulp.
- Cell-free zone decreases in size when dentin formation occurs at a rapid rate.
- The cell-free zone consists of a network of nerve fibres which lost their myelin sheath. This is known as Plexus of Rashkow.
Written by Anisha Valli
Sunday, June 17, 2018
Mnemonics for special orthopedic tests
1) TEST: BRUDZINSKI 'S SIGN --
*Description: Flexion of neck elicits reflexive flexion of knee.
*Significance: suggests meningitis.
* Mnemonic : a) Imagine as if the patient is in SKI position on the bed (neck and knee flexed) .
b) The neck is stiff from the freezing in the snow.
b) The neck is stiff from the freezing in the snow.
2) DIX HALLPIKE MANEUVER --
*Significance : suggests BPPV.
*Mnemonic : Spike your drink and see the hall spin around you (vertigo) .
3) FINKELSTEINS 'S TEST :
* Significance : for dequervain's tenosynovitis .
*Mnemonic : a) Ask the patient to flick a coin of ten.
b) The head's side of the coin has de (the) queen embossed on it.
b) The head's side of the coin has de (the) queen embossed on it.
4) HAWKIN'S TEST :
*Description : Internally rotate the shoulder to produce pain if rotator cuff pathology.
*Mnemonic :Imagine a hawk flying in circles (rotate) , waiting to attack the shoulder of its prey.
*Description : Internally rotate the shoulder to produce pain if rotator cuff pathology.
*Mnemonic :Imagine a hawk flying in circles (rotate) , waiting to attack the shoulder of its prey.
5) LHERMITTE'S SIGN:
*Description : Passive forward flexion of head causes electric sensation down the spine.
*Description : Passive forward flexion of head causes electric sensation down the spine.
*Mnemonic : Imagine a hermit (sadhu) giving his blessings (aashirwaad) which induces some electric power down your body.
6) LACHMAN TEST:
*Significance : indicates anterior cruciate ligament injury.
*Mnemonic : Imagine anterior cruciate ligament to be a latch which keeps the tibia and femur locked to each other.
7) O'BRIEN TEST:
*Description : With shoulder at 90 degrees flexion, instruct patient to point thumb at ground and resist downward force. Repeat with palm facing upwards.
*Description : With shoulder at 90 degrees flexion, instruct patient to point thumb at ground and resist downward force. Repeat with palm facing upwards.
*Significance : Pain suggests labral tear.
*Mnemonic : a) This is a story of O'Brien who worked as a labourer.
b) He got thumbs down for his work.
c) So he had to beg (with palms facing upwards) to make end's meet.
*Mnemonic : a) This is a story of O'Brien who worked as a labourer.
b) He got thumbs down for his work.
c) So he had to beg (with palms facing upwards) to make end's meet.
8) SPURLING TEST
*Significance : Tingling or pain along cervical nerve root suggests cervical radiculopathy.
*Mnemonic :a) Spurling test is for spine.
b) Imagine if there are spurs formed in spine, they will compress the spinal cord causing radiculopathy.
b) Imagine if there are spurs formed in spine, they will compress the spinal cord causing radiculopathy.
9) McMURRAY'S TEST :
*Significance : positive test suggests meniscal tear.
* Mnemonic : a) Tennis players are very vulnerable to meniscal tear.
b) Imagine Andy Murray to be suffering from meniscal tear.
c) Also Mc Murray and meniscus both have M and C.
b) Imagine Andy Murray to be suffering from meniscal tear.
c) Also Mc Murray and meniscus both have M and C.
10) PHALEN 'S TEST :
*Description : Instruct patient to bring dorsal aspect of hands together.
*Significance : Tingling or paresthesia in lateral 3.5 fingers suggests carpal tunnel syndrome.
*Description : Instruct patient to bring dorsal aspect of hands together.
*Significance : Tingling or paresthesia in lateral 3.5 fingers suggests carpal tunnel syndrome.
* Mnemonic : a) Imagine a felon who is handcuffed with dorsal aspect of his hands together.
b) The handcuffs are tight and compressing his median nerve causing tingling and numbness.
b) The handcuffs are tight and compressing his median nerve causing tingling and numbness.
Submitted by Abuzar Asif
Sunday, June 10, 2018
Mnemonics and basics of ECG interpretation
Hello !!
Many people think ECG interpretation is hard i will take you through the basics of it.
To understand how to interpret the ECG you must first understand the basics which is out of the scope of this scope.
To interpret an ECG the following are the most important:
1. Understanding the basics
2. Systematic approach for interpretation
SOME BASICS
ECG WAVEFORMS
- What do the waves represent ?

Adapted from: https://meds.queensu.ca/central/assets/modules/ts-ecg/waves_and_complexes.jpg
WAVES AND INTERVALS PICTORIAL REPRESENTATION

Adapted from: https://ecgwaves.com/topic/ecg-normal-p-wave-qrs-complex-st-segment-t-wave-j-point/
- What do the boxes represent ?
Each small box in the ECG paper is 1 mm = 0.1 mV = 0.04 secs
Each large box in the ECG paper is 5mm = 0.5 mV = 0.20 secs (0.04 X 5)
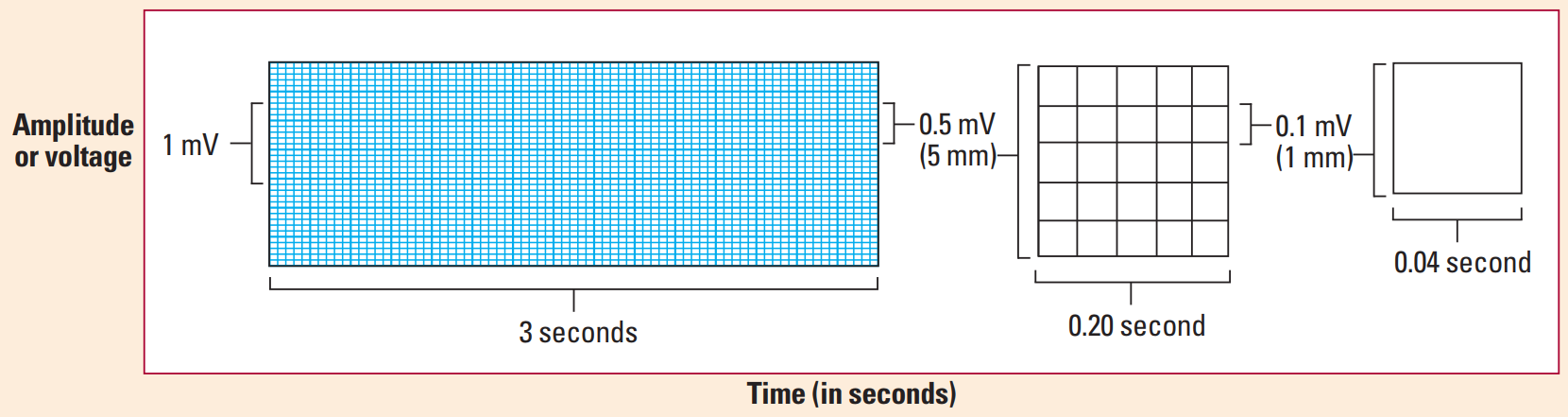
Adapted from: ECG interpretation made incredibly easy —5th ed
SYSTEMATIC INTERPRETATION
1. Heart rhythm
- Use paper and pencil/pen method for determination of the heart rythm
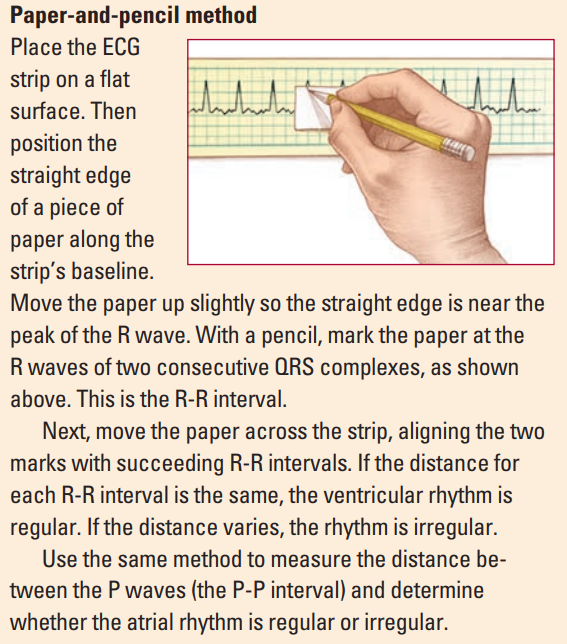
Adapted from: ECG interpretation made incredibly easy —5th ed
- Determine whether it is a sinus rhythm ? (in which each QRS complex is preceded by a p wave)
- Determine whether the rhythm is regular or not:
- Types of rhythms:
a. Regularly regular rhythm: In a normal individual
b. Regularly irregular rhythm: Sinus arrhythmia
c. Irregular irregular rhythm: Atrial fibrillation
2. Heart Rate
- Atrial rate : between 2 P waves
- Ventricular rate : between 2 R waves
- Can be calculated depending on whether the rhythm is regular or irregular
- If the rhythm is regular the following methods can be used:
a. 300 method
In this take 300 divided by number of large boxes between 2 R waves
Example: If the number of boxes between 2 R waves is 3 then the Rate would be 300/3 = 100 beats/min.
b. 1500 method
In this take 1500 divided by the number of small boxes between 2 R waves
Example: If the number of boxes between 2 R waves is 14 then the Rate would be 1500/14 = 107 beats/min.
c. Rapid estimation method
Use this only if the rhythm is regular
Using the number of large boxes between R waves or P waves as a guide, you can rapidly estimate ventricular or atrial rates by memorizing the sequence “300, 150, 100, 75, 60, 50.”

For an Irregular rythm:
- Use the rythm strip / Lead II and count the number of R waves in 6 seconds (30 large boxes ) and multiply by 10.
- Use the rythm strip / Lead II and count the number of R waves in 6 seconds (30 large boxes ) and multiply by 10.
3. Cardiac Axis
- Determined using lead I and II / aVF
- Determine the cardiac axis : the easiest way is to use the thumb rule
- Left thumb represents lead 1
- Right thumb represents lead 2 or lead aVF

- Mnemonics for the causes of axis deviation RAD RALPH the LAD from the VILLA
RAD - Right axis deviation causes
R- Right ventricular hypertrophy
A- Anterolateral MI
LPH- Left posterior hemiblock
LAD - Left axis deviation
V- Ventricular tachycardia
I- Inferior MI
L- Left ventricular hypertrophy
LA- Left Anterior fascicular block
4. Evaluate P wave
- P waves should be upright in leads I and II, inverted in aVR
- Are p waves present before every QRS complex? if yes; sinus rhythm
- P waves may be absent in; atrial fibrillation
- Normal P wave : <0.10 sec (2.5 small boxes)
- Common Abnormalities of P wave
Bifid/notched P waves (p mitrale) : Left atrial enlargement - classically due to mitral stenosis
Peaked P waves (p pulmonale) : Right atrial enlargement - due to Pulmonary Hypertension
5. Duration of PR interval
- The PR interval is the time from the onset of the P wave to the start of the QRS complex
- It reflects conduction through the AV node
- Normal duration : 3-5 small boxes (0.12 to 0.20 secs)
- Determine if the duration is normal
- Common abnormalities of PR interval
a. Can be prolonged in: AV block
b. Can be short in: Pre-excitation syndromes e.g in Wolff-Parkinson-White syndrome; which involve the presence of an accessory pathway connecting the atria and ventricles.The accessory pathway conducts impulses faster than normal, producing a short PR interval.
6. Duration of the QRS complex
- Normal duration : 2-3 small boxes (0.08-0.12 secs)
- Determine if the duration is normal
- Are all QRS complexes of same size and shape ?
- Does a QRS complex appear after every p wave ? if not consider an AV block (second degree AV block); in which the PR-interval progressively gets longer until a QRS is dropped and only the p-wave is present
- Common abnormalities of QRS complex
a. QRS deflections; Exaggerated QRS deflections indicate ventricular hypertrophy
- The voltage criteria for left ventricular hypertrophy are fulflled when the sum of the S and R wave deflections in leads V1 and V6 exceeds 35 mm (3.5 mV) ( 7 large boxes )
- Right ventricular hypertrophy causes tall R waves in the right ventricular leads (V1 and V2)
- Diminished QRS deflections occur when pericardial effusion or obesity electrically insulates the heart
b. Narrow QRS complex morphology (<0.08 secs)
- Atrial flutter
- Junctional tachycardia
- Note : normal sinus rhythm also has a narrow QRS complex morphology
c. Broad/wide complex QRS complex morphology (>0.12 secs)
- Bundle branch block (BBBB) : LBBB or RBBB
- Hypokalemia
- Poisoning with sodium-channel blocking agents (e.g. tricyclic antidepressants) - remember this also gives you a dominant R wave in lead avR.
7. ST segment
- The ST segment is the flat, isoelectric section of the ECG between the end of the S wave and the beginning of the T wave.
- It represents the interval between ventricular depolarization and re polarization.
- The most important cause of ST segment abnormality (elevation or depression) is myocardial ischemia or infarction.
The causes of ST elevation can be remembered using the mnemonic ELEVATION
Electrolyte abnormalities
Left bundle branch block
Aneurysm of left ventricle
Ventricular hypertrophy
Arrhythmia disease (Brugada syndrome, ventricular tachycardia)
Takotsubo/Treatment (iatrogenic pericarditis)
Injury (myocardial infarction/ischaemia or cardiac contusion)
Osborne waves (hypothermia or hypocalcemia)
Non-atherosclerotic (vasospasm or Prinzmetal’s angina)
The causes of ST depression can be remembered using the mnemonic DEPRESSED ST
Drooping valve (MVP)
Enlargement of LV with strain
Potassium loss (hypokalemia)
Reciprocal ST- depression (in I/W AMI)
Embolism in lungs (pulmonary embolism)
Subendocardial ischemia
Subendocardial infarct
Encephalon haemorrhage (intracranial haemorrhage)
Dilated cardiomyopathy
Shock
Toxicity of digoxin, quinidine
8. Evaluate T wave
It represents ventricular repolarisation
NB:
Upright in all leads except aVR and V1
Amplitude <5mm (5 small boxes) in limb leads, <15mm (3 large boxes) in precordial leads
- Are T waves present ?
- Do they have normal shape ?
- Do they have normal amplitude?
- Do they have same deflection as QRS complexes ?
- Common T wave abnormalities
a. Inverted T wave
- Can be remembered by the mnemonic INVERT
Ischemia, raised ICP
Normality [esp. young, black]
Ventricular hypertrophy
Ectopic foci [e.g. calcified plaques], classic pulmonary Embolism
RBBB, LBBB
Treatments [digoxin]
b. Tall/peaked T waves
- Classically seen in Hyperkalemia
c. Hyperacute T waves
- Seen in early stages of ST elevation MI (STEMI)
d. Biphasic T waves
-Ischaemic T waves go up then down
-Hypokalaemic T waves go down then up
e. Flat T wave
- Ischaemia
- Hypokalemia
9. Determine the duration of the QT interval
QT interval : is the time from the start of the Q wave to the end of the T wave. It represents the time taken for ventricular depolarisation and repolarisation, effectively the period of ventricular systole from ventricular isovolumetric contraction to isovolumetric relaxation
- QT interval is inversely proportional to heart rate i.e as the HR increases the QTi decreases and vice versa
- The QT interval should be measured in either lead II or V5-6
- Determine if the QT interval is normal ? (normal = 0.36 to 0.44 secs = 9-11 small boxes)
- Corrected QT interval (QTc)
-- Due to the variations of the heart rate : The corrected QT interval estimates the QT interval at a heart rate of 60 bpm.
-- The following formula can be used to calculate the QTC = QT interval / √ RR interval (Bazzet's formula)
-- RR interval = 60/Heart rate
-- Note: there are many formulas which can be used for calculation of but this is probably the easiest one.
-- QTc is prolonged if > 0.44 secs in men or > 0.46 secs in women
-- QTc > 500 is associated with increased risk of torsades de pointes
-- Due to the variations of the heart rate : The corrected QT interval estimates the QT interval at a heart rate of 60 bpm.
-- The following formula can be used to calculate the QTC = QT interval / √ RR interval (Bazzet's formula)
-- RR interval = 60/Heart rate
-- Note: there are many formulas which can be used for calculation of but this is probably the easiest one.
-- QTc is prolonged if > 0.44 secs in men or > 0.46 secs in women
-- QTc > 500 is associated with increased risk of torsades de pointes
- Causes of prolonged QTc > 0.44 secs
Hypokalaemia
Hypomagnesaemia
Hypocalcaemia
Hypothermia
Myocardial ischemia
Post-cardiac arrest
Raised intracranial pressure
Congenital long QT syndrome
Drugs - quinidine, amiodarone, TCA's
- Causes of a short QTc < 0.36 secs
Hyperkalemia
Hypercalcaemia
Congenital short QT syndrome
Digoxin effect
The End !!
Please note that this is not everything that you need to know , and this article doesn't cover everything about the ECG, it just covers the basics and the most common abnormalities that can be found on an ECG.
But for sure ! It has just enough information which can help anyone understand and interpret and ECG.
Mohammad Farouq,
Final year medical student, MUHAS.
Friday, June 8, 2018
MCQ Mnemonic Series: Apple jelly nodules
#ENT
#Dermatology
Apple jelly nodules on nasal septum are seen in :
Options:
A) Leprosy
B) Syphilis
C) Lupus vulgaris
D) Wegner’s granulomatosis
✍✍✍✍
LLuPPus vulgaris
aPPLLe jelly nodules
{Luppal ~ Apple)
By
Dr. Shubham Patidar
Letters of Recommendation [LORs] 101
The letters of recommendation are very important for the residency application process. All the programs require a minimum of three and a maximum of four letters of recommendation for a complete application. So, I thought I will put together all the information needed to know about Letters of Recommendation[LORs].
DISCLAIMER: Long post!!
1. How important are LORs?
LORs are compulsory while applying for a residency program. Most of the programs require at least three LORs for a complete application.
2. Do all the LORs need to be from the states?
It is good to have all the LORs from the clinical experience from the states. But, a few programs require a letter from the department head of your med school. In such cases, you need to submit one from your med school.
If you don’t have all the LORs from the states, try to get at least two. Its easier for the program director to believe if someone from the same country says that you are well versed with the system than from someone who is outside the country.
But is there not anyone who matched without any letters from the states? There are!! But there are many terms and conditions involved like stellar scores, strong contacts etc. So, to be on the safe side it's better to apply with letters written by someone in the states.
3. What is the difference between a waived LOR and non-waived LOR?
Waived LOR is uploaded by the LOR writer or someone on his behalf and it by default means you never saw the letter.
Non-Waived LOR is uploaded by you or the letter writer. It means that you have seen the letter and know the contents.
Waived LORs are supposed to carry more value than non-waived. But, if you believe that a non- waived LOR is stronger than a different waived LOR you have, definitely use the strong one.
Value: strong waived LOR> strong Non-waived LOR> weak waived LOR>weak Non-waived LOR.
4. How do I send a request/upload a LOR into the ERAS?
There is a tab for LORs on ERAS. Follow the instructions and it gives a printable form to send to the LOR author to upload the letter. You can also send the request directly via ERAS to the author. It has step by step process on how to upload a LOR.
Remember the author should have an AMA account to upload.
5. When do I ask for a LOR?
Usually in the last week or last day of your rotation. Ask your author for a feedback first and assess what he/she feels about you and then ask for a LOR.
Example:
“Hi doctor, it has been a pleasure working with you. I would like to take any feedback you have for me regarding my performance”
“I will be applying for so and so residency this year, will you be comfortable in writing a strong LOR for me?”
If they say yes, ask them if they are comfortable uploading it to ERAS and if they are familiar with it.
Tell them you will send the ERAS request form once the application season starts. If they are not, offer to help them upload the letter explaining to them the importance of a waived LOR.
Never push them to do what they are not comfortable with. Be polite.
6. My LOR author offered me to write my own LOR, what do I do?
Never leave such an opportunity. It means that the mentor trusts you to write a letter. This is an opportunity to write a strong LOR. Try to include the following in the LOR:
A) Start with how the author knows you and how long he/she worked with you.
B) Try to give examples to the positive features described. Ex: Don’t say this student is punctual, say something like he/she always arrived before time and left only after the work is done. It will show you are punctual and committed.
C) Put in strong adjectives. Ex: Rather than hardworking say very hardworking.
Keep a proforma in handy. Some authors might ask proforma. Try to personalize as much as you can.
7. I did a lot of rotations and have a lot of LORs, which ones do I use?
This usually happens with repeat applicants. First of all, use the LORs which you feel are the strongest. If you believe that all of them are strong enough, use the LORs specifically from the same region as the program. Ex: If you are applying to programs in Michigan, and if you happen to have a LOR written by someone in Michigan-use it.
If any your LORs are from people in higher positions like PD, APD, Chairman and are strong LORs- use them.
8. How do I get my LORs from the previous year?
Just buy the token and login into your ERAS account, LORs would have been transferred.
9. I have a LOR from a specialty different from what I am applying for, Is it useful?
Yes! Although it is better to have a LOR from the same specialty, it is not bad to have LOR from a different specialty.
Any LOR is better than no LOR. But make sure that LOR doesn’t say that you are interested in a specialty different from the one you are applying to. Or ask your LOR author to mention your dedication to the specialty you are applying for.
Ex: If a pediatrics author is writing LOR for IM application, Ask them to mention you are dedicated for IM and not to mention you like peds.
10. How useful are the letters of reference?
Letters of reference are written by a physician who you didn’t work with but know you personally. This is a gray area. It worked for some people and some consider it useless.
TIPS:
1. Use google to find proformas online. Don’t copy paste but try to understand the format.
2. Try to send it to people who matched, they might help you make corrections and make it stronger.
3. Authors might not upload the same LOR you gave them. Remember, they have the liberty to change-they are the authors.
4. If someone offers you to write a LOR after September, ask them to write it and take it by hand to interviews and give it to the PDs. Most PDs will e interested in reading them and will appreciate the effort taken by your mentor. It is a bigggg plus.
5. If your rotations happened well before application season, stay in touch with your mentor through Emails, tell them about your progress. Once the application season begins, remind them of the LOR.
6. ERAS takes a maximum of two weeks to process the LOR during peak times. So, keep that in mind. Don’t keep them not uploaded till the last minute.
7.If your author is not uploading the LOR on time send them Emails with subject “gentle reminder” beginning July 15th and tell them they have to upload by September 1st or else you might not be able to apply for residency. Remember they are very very busy.
This whole information is through personal experience and from questions I usually find online. Hope this compilation helps. Feel free to ask questions or contribute to this. 😊
Give as you live <3
Much love <3
-Hyndavi
Thursday, June 7, 2018
How to choose which residency programs to apply to?
Match season is coming and everyone is asking: What programs should I apply to :D ?
Well, there is no magical answer for this and each applicant has his/her own situation.
Below are some sources that may help in gathering some info about programs:
1- www.Matcharesident.com
This paid (79$) website provides a list of programs that you are eligible to apply to after filling the following requirements: USMLE scores, Visa Status, AMG or IMG, time since graduation, having US clinical experience or not and of course the specialty you are applying for.
It gives you a list of the programs, arranged alphabetically according to state with USMLEs and year of graduation cut-offs in addition to “IMG-friendliness” of the program among many other factors.
2- ERAS (Electronic Residency Application Service)
ERAS itself will show you all the programs available but without any filters, so you will need to check the website of each program individually to avoid applying for nothing. For example, ERAS won’t stop you from applying to a program in California even if you don’t have a PTAL - which is a requirement for all California programs.
Keep in mind is ERAS is the place where you apply to programs, so regardless of any source you use to create your list, ERAS is the final destination to choose programs from.
3- Website of each program
One of the most reliable ways to know about a program is to check the website itself. You ll find the info you need mostly under the name/title/tab of: Prospective Applicants or How to Apply and sometimes in the FAQ section.
Unfortunately, some programs websites are deficient and not organized or not even accessible. In this case, you ll have to use the other sources mentioned in this post to get the info you want.
4- FRIEDA (Fellowship and Residency Electronic Interactive Database)
FRIEDA is an online database of all graduate medical education programs in the United States that are accredited by the Accreditation Council for Graduate Medical Education
Click here to access FRIEDA or just search FRIEDA on Google. Make an account and enjoy searching. You can use filters like: states, visa sponsorship..etc.
5- Doximity
Doximity is an online social networking service for U.S. clinicians. You can create an account and see programs in different specialties arranged according to research output or reputation and US news ranking.
6- Already made lists
You ll find many lists circulating around the internet. You may use them too but an advise it to double check them and make sure that they are uptodate since programs policies may change over the years.
7- Asking seniors
Seniors may help and give you a more detailed insight about programs and states. Ask them :)
==
Tips:
> In order to apply to California programs, you need what is so-called: a PTAL ( Postgraduate-Training Accreditation Letter). For more information, click here.
> The situation may be different in different specialties. For instance, Peds has less than 200 programs which means searching will need less time and effort than IM which has 400+ progs!
> It is good to use more than one source. You can use matcharesident list in addition to checking ERAS and the website of each program. Matcharesident may rarely miss a program and sometimes programs show up late in ERAS.
> Search well and specify some good time to search programs. This is a very important decision that may affect the rest of your life :D
> Apply to all programs in a particular geographical location if you have a strong family tie and you REALLY want to match there. DO NOT MISS OUT ON ANY PROGRAM IN THAT CITY/STATE.
Wishing you a good Match season everyone :)
-Murad
Well, there is no magical answer for this and each applicant has his/her own situation.
Below are some sources that may help in gathering some info about programs:
1- www.Matcharesident.com
This paid (79$) website provides a list of programs that you are eligible to apply to after filling the following requirements: USMLE scores, Visa Status, AMG or IMG, time since graduation, having US clinical experience or not and of course the specialty you are applying for.
It gives you a list of the programs, arranged alphabetically according to state with USMLEs and year of graduation cut-offs in addition to “IMG-friendliness” of the program among many other factors.
2- ERAS (Electronic Residency Application Service)
ERAS itself will show you all the programs available but without any filters, so you will need to check the website of each program individually to avoid applying for nothing. For example, ERAS won’t stop you from applying to a program in California even if you don’t have a PTAL - which is a requirement for all California programs.
Keep in mind is ERAS is the place where you apply to programs, so regardless of any source you use to create your list, ERAS is the final destination to choose programs from.
3- Website of each program
One of the most reliable ways to know about a program is to check the website itself. You ll find the info you need mostly under the name/title/tab of: Prospective Applicants or How to Apply and sometimes in the FAQ section.
Unfortunately, some programs websites are deficient and not organized or not even accessible. In this case, you ll have to use the other sources mentioned in this post to get the info you want.
4- FRIEDA (Fellowship and Residency Electronic Interactive Database)
FRIEDA is an online database of all graduate medical education programs in the United States that are accredited by the Accreditation Council for Graduate Medical Education
Click here to access FRIEDA or just search FRIEDA on Google. Make an account and enjoy searching. You can use filters like: states, visa sponsorship..etc.
5- Doximity
Doximity is an online social networking service for U.S. clinicians. You can create an account and see programs in different specialties arranged according to research output or reputation and US news ranking.
6- Already made lists
You ll find many lists circulating around the internet. You may use them too but an advise it to double check them and make sure that they are uptodate since programs policies may change over the years.
7- Asking seniors
Seniors may help and give you a more detailed insight about programs and states. Ask them :)
==
Tips:
> In order to apply to California programs, you need what is so-called: a PTAL ( Postgraduate-Training Accreditation Letter). For more information, click here.
> The situation may be different in different specialties. For instance, Peds has less than 200 programs which means searching will need less time and effort than IM which has 400+ progs!
> It is good to use more than one source. You can use matcharesident list in addition to checking ERAS and the website of each program. Matcharesident may rarely miss a program and sometimes programs show up late in ERAS.
> Search well and specify some good time to search programs. This is a very important decision that may affect the rest of your life :D
> Apply to all programs in a particular geographical location if you have a strong family tie and you REALLY want to match there. DO NOT MISS OUT ON ANY PROGRAM IN THAT CITY/STATE.
Wishing you a good Match season everyone :)
-Murad
Subscribe to:
Posts (Atom)