Hey Awesomites
Cincinnati Pre - Hospital Stroke scale is one of the most common scale to detect stroke early on. Remember the mnemonic - FAST

Friday, March 16, 2018
Writing a personal statement for residency
Your personal statement (PS) should be your experiences, what make you who you are.
Think of it this way - if you were to sum up your life in one page, how would you do it?
How do you let a person "meet" you without actually meeting you?
How do you put things that are not in your CV on your application?
That's your personal statement my friend.
Now there are many tips on the internet on how to write a personal statement - these are mine and what I found helpful.
Think of it this way - if you were to sum up your life in one page, how would you do it?
How do you let a person "meet" you without actually meeting you?
How do you put things that are not in your CV on your application?
That's your personal statement my friend.
Now there are many tips on the internet on how to write a personal statement - these are mine and what I found helpful.
Femoral triangle and femoral sheath contents mnemonic
Hello!
The femoral triangle is a subfascial space bounded superiorly by the inguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle.
Contents of the femoral triangle mnemonic:
The femoral triangle is a subfascial space bounded superiorly by the inguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle.
Contents of the femoral triangle mnemonic:
Authors diary: Octopus and tyrosinase
Hey everyone!
Here's another way I study - when I am looking up cool things in other creatures, I compare it to the human body. It's fun!
Here's another way I study - when I am looking up cool things in other creatures, I compare it to the human body. It's fun!
Wednesday, March 14, 2018
Pursuing ophthalmology in India
Since my mom first introduced me to the slit lamp view of the eye and dad to the indirect ophthalmoscopy, I developed a liking for ophthalmology. The magnified view of the eye through the slit lamp just looks 'oh so beautiful' and it's such a fun challenge to master indirect ophthalmoscopy- I didn't think much in the counselling room while 'locking' the MS Oph option. Also, the fact that you have to work with all the cool gadgets and gizmos, lasers and stuff made me incline towards it.
Ophthalmology is a mutifaceted branch. Those who are into diagnostics and literature get their own share as well as those who want to take matters into their own hands and like to cut,paste, and remove things. The puzzle of diagnosis and the thrill of surgery, both can be had here.
Though not as demanding as general medicine or surgery, ophthalmic surgeries like cataract have a steep learning curve,a personal opinion of mine. But when you make sure that all the things fall into places rightly, it is highly satisfying an experience. The patient's smile the next day when they see clearly feels so good to the heart.
Experience in residency varies per college. I for one am happy with mine. I have done a few basic surgeries like pterygium and dacryocystectomy independently but under supervision during my first year itself. Currently, I'm working on tunnel making in cataract surgery.
I have seen a lot of interesting cases of lids, cornea, and the fundus.
At times though, performing sac syringing of every pre op patient and filling up of discharge cards of the post op patients makes me go meh. But this is just nitpicking, I have a fair idea about the extreme workload of redundant stuff in other colleges.
After passing out, there are many fellowship programs offered by institutions. Getting a fellowship done is sort of a norm nowdays.
As mentioned before, this is an investment intensive branch, one needs to continually upgrade their machines and bring in new ones
if interested in establishing a privately owned set up. A job in an institution can be an option but things may get pushy or so I've heard.
Summing it up, this is like a cute little baby who is rather tough to please, but when you get it right, the smile is priceless.
How to leave a good impression during your clinical rotations?
Many of us are looking for observerships/electives in the US to gain some clinical experience, have recommendation letters and become more familiar with the medical system in USA.
In this post, I will shine the light on some points that will help in getting the maximum benefit from your rotations.
So, Let’s go:
1- Always come early and show commitment
If the working day starts at 7:30 am, be there at 7:20 am.
2- Dress properly
>Many hospitals have a dress-code, this is usually mentioned in the paperwork that you have to read/fill.
Eg: Business casual; shirts, ties and no jeans for men.
>Take care of your personal hygiene, use deodorants....etc
3- Write down notes
Have a small notebook and a pen. Write new cases that you see or any interesting syndrome. When you go back home, read more about these cases and check if there are any new scientific papers about them.
4- Be proactive
Don’t just sit and do nothing. Ask questions and check if you can present a case / give a talk or a presentation. Especially if you are doing an observership, the outcome at the end can really vary depending on how you use your time and how you reflect yourself as a doctor.
5- Know when to ask questions
It is nice to know more and to show interest but avoid the times when residents/fellows are busy, these include but are not limited to: pre-rounding, immediately after rounds when orders will be entered.
6- Don’t be “Mr. Know-it-all”
Although answering questions is important and can give a very good idea about you. Acting snobby and answering everything including questions that are directed to the residents may have an opposite effect.
Be patient and don’t interrupt. Answer when the question is directed to you or when it is open to everyone to answer.
7- Identify important "players"
Get to know who is the program director, the associate program director, attendings who are known to write good recommendation letters and those who are not. You will find a resident/senior/fellow who will provide this piece of info.
After all, you need to be remembered and to have a good recommendation letter when you apply for the match so do your best go get one! A strong recommendation letter from a chairman has much more weight than an average one from a newly appointed attending!
8- Be social
Respect everyone, smile, shake hands and introduce yourself to people who you meet for the 1st time. It is also cool to have nice conversations outside the field of medicine. For example, movies, books and sports. This will give an idea that you are well-rounded and more approachable rather than just an outsider who is there to do a job.
9- Discover the place
Try to be familiar with the hospital, its departments, the floors and the outpatient clinics. This will lessen the moments - especially during the first week of the rotation - when you will suddenly stop, conclude that you are lost and start blankly looking around :D
10- Remember that the first impression is vital and very hard to change, so be sure that the first impression that is made about you is positive.
In short, just be yourself and give it your best shot :)
Good luck everyone!
PS: this post is subjective to updates whenever I remember any new point that will help :)
-Murad
In this post, I will shine the light on some points that will help in getting the maximum benefit from your rotations.
So, Let’s go:
1- Always come early and show commitment
If the working day starts at 7:30 am, be there at 7:20 am.
2- Dress properly
>Many hospitals have a dress-code, this is usually mentioned in the paperwork that you have to read/fill.
Eg: Business casual; shirts, ties and no jeans for men.
>Take care of your personal hygiene, use deodorants....etc
3- Write down notes
Have a small notebook and a pen. Write new cases that you see or any interesting syndrome. When you go back home, read more about these cases and check if there are any new scientific papers about them.
4- Be proactive
Don’t just sit and do nothing. Ask questions and check if you can present a case / give a talk or a presentation. Especially if you are doing an observership, the outcome at the end can really vary depending on how you use your time and how you reflect yourself as a doctor.
5- Know when to ask questions
It is nice to know more and to show interest but avoid the times when residents/fellows are busy, these include but are not limited to: pre-rounding, immediately after rounds when orders will be entered.
6- Don’t be “Mr. Know-it-all”
Although answering questions is important and can give a very good idea about you. Acting snobby and answering everything including questions that are directed to the residents may have an opposite effect.
Be patient and don’t interrupt. Answer when the question is directed to you or when it is open to everyone to answer.
7- Identify important "players"
Get to know who is the program director, the associate program director, attendings who are known to write good recommendation letters and those who are not. You will find a resident/senior/fellow who will provide this piece of info.
After all, you need to be remembered and to have a good recommendation letter when you apply for the match so do your best go get one! A strong recommendation letter from a chairman has much more weight than an average one from a newly appointed attending!
8- Be social
Respect everyone, smile, shake hands and introduce yourself to people who you meet for the 1st time. It is also cool to have nice conversations outside the field of medicine. For example, movies, books and sports. This will give an idea that you are well-rounded and more approachable rather than just an outsider who is there to do a job.
9- Discover the place
Try to be familiar with the hospital, its departments, the floors and the outpatient clinics. This will lessen the moments - especially during the first week of the rotation - when you will suddenly stop, conclude that you are lost and start blankly looking around :D
10- Remember that the first impression is vital and very hard to change, so be sure that the first impression that is made about you is positive.
In short, just be yourself and give it your best shot :)
Good luck everyone!
PS: this post is subjective to updates whenever I remember any new point that will help :)
-Murad
Tuesday, March 13, 2018
My USMLE Step 1 Experience ( Road to 255 )
Hello everyone :) I would like to share with you what I did/studied for USMLE Step 1
It is gonna be long because I tried to include every single question that I was asked about my prep
First of all, I would like to thank everyone who I met during this journey from all over the world, Thank you everyone!
Sources used for studying:
>First Aid
>First aid proposed and official errata (please check the proposed errata before studying any page in First Aid, it may have nice mnemonics, corrections. concepts..etc):
*https://www2.usmle-rx.com/proposed-errata-and-suggestions-fa-step-1
*https://firstaidteam.com/updates-and-corrections/
>Uworld
>Uworld biostat review
> +/- kaplan epidemiology part for step 2 ( those 2 youtube videos may be used in addition to kaplan):
https://www.youtube.com/watch?v=75pQPB1RF50
https://www.youtube.com/watch?v=VMI9UuNqoGI
>Pathoma
>a person rearranged Pathoma into this amazing Onenote website:
https://onedrive.live.com/view.aspx?cid=375c2c99998a5c62&page=view&resid=375C2C99998A5C62!2705&parId=375C2C99998A5C62!2703&authkey=!AHH10BbZMBrqM0k&app=OneNote
>Sketchy micro and pharm videos ( I didn’t watch all videos but a lot them are really helpful)
>Kaplan videos for biochem / Sam Turco
>Kaplan step 2 patient safety chapter
>Conrad fischer 100 ethics cases
>+/- Flashcards notes ( Brosencephalon Anki deck for revision for some First Aid chapters)
>+/- BRS physio (curves and their questions in cardiology/respiratory)
Method of studying:
>Did First aid general principles part except biochem
Did some systems then went back to biochem
Then completed the systems
>Uworld mainly done after first solid read of First Aid ( I started doing Uworld after finishing some of First Aid then I stopped and continued studying First Aid)
>I didn’t do any online NBME but I solved NBME 15 16 17 18 and biostat and genetics questions in older NBMEs
Also did UWSA 1, 2 and FRED
(I felt my level was ok, I don’t advice you to do this..do 2 online NBMEs at least. I also didn’t try to convert my offline score and compare it..again, don’t do what I did :D)
==============================================
==============================================
First Aid and Uworld are used for all the subjects in addition to what is mentioned below:
- Biochem:
>Kaplan Biochem Videos by Dr. Sam Turco
>Kaplan biochem book for pages that correspond to the videos only..fast skimming, don’t spend much time doing it!
- Immuno:
>https://www.youtube.com/watch?v=T_4TrNRa3v8
>https://mynotes4usmle.tumblr.com/post/74125122501/anticancer-drugs-no-bms-mnemonic#.WnqBQZx97IU
>https://mynotes4usmle.tumblr.com/post/95332165430/immunosupressants-drug-mnemonic-bc-everythings#.WnqB-Zx97IU
- Micro:
>Sketchymicro videos +/- pdf file of videos helps to cement info
>Use a lot of mnemonics whether from the proposed errata or any other source you find, also take care of the pics of organisms because they can be a question too.
> viruses DNA vs RNA and taxonomy mnemonic:
https://www.youtube.com/watch?v=Df_qAFF58Ec&t=1s
The video is drawn in a nicer way here too:
https://www.youtube.com/watch?v=rgz_3Yjw0vY
- General Patho:
Pathoma
- General Pharm:
Dr Raymond in Kaplan pharm about energy and inhibitors
- Public Health Sciences:
>Biostat: the more questions you solve the better, as mentioned above: uw biostat review
>+/-Kaplan step 2 epidemiology may help in giving a broader idea for a person who is studying biostat for the 1st time
>Conrad 100 ethics cases + behavioral:Kaplan step 2 patient safety chapter
- Cardiology:
-Embryology:
https://www.youtube.com/watch?v=YxPp67XluQA&t=6s
-Physiology:
BRS Physio - Cardio chapter ( if needed)
-Pathology:
Pathoma
-Pharmacology:
Some mnemonics that may help in hyperdyslipidemia:
> https://www.youtube.com/watch?v=fTA5HOa87pM
> https://www.youtube.com/watch?v=HOXSaGpiSuo&t=3s
>http://www.medicowesome.com/2013/08/how-to-remember-lipoprotein-disorders.html
Antiarrythmics:
> http://www.medicowesome.com/2014/10/antiarrhythmic-drug-classes-mnemonic.html
>http://usmle1mikmonics.tumblr.com/post/81324508295/bacman-class-1-antiarrhythmic-na-blockers
- Endocrine:
-Physiology:
+/-BRS Physio
-Pathology
Pathoma
-Pharmacology
Sketchypharm..some really nice videos for anti-Diabetic drugs
- GI:
Pathology:
Pathoma
- Hemonc:
>Pathology and a lot of physio:
Pathoma
>Pharmacology:
In addition to many mnemonics that are found online, you may check the anti-Neoplastic part of Sketchy pharm, I haven’t seen it but I heard it is cool.
- Musculoskeletal:
Pathology:
Pathoma
- Neuro:
Anatomy:
>Some books in First Aid are not clear enough ..eg: the foramina of the skull,,I suggest looking for some pics that are not clear in First Aid.
> A much simpler way to understand Basal Ganglia:
https://www.youtube.com/watch?v=-5PXAUdWDgU
(the whole channel: “Draw it to know it” is amazing)
>An amazing video to memorize the Brachial plexus:
https://www.youtube.com/watch?v=gTas7ijp0YE&t=328s
>Sleeping associated neurotransmitters
https://mynotes4usmle.tumblr.com/post/74247543467/neurotransmitters-associated-with-sleep-mnemonic
Pathology:
Pathology:
Pathoma presents tumors in a simpler way
- Psych:
I suggest studying drug toxicities, DSM rules and drugs mech of action from Uworld because it is more arranged and accurate than First Aid.
- Renal:
Patho and some physio:
Pathoma is great in pathology here and some parts of physiology are covered too
- Reproductive:
>Physio:
Mnemonic for tanner staging:
https://mynotes4usmle.tumblr.com/post/152650094930/tanner-stages-of-development-mnemonics
>Patho:
The tumors part can be rearranged better in First Aid, I suggest focusing on Pathoma and checking the reproductive part here too, tables can really make things easier:
https://onedrive.live.com/view.aspx?cid=375c2c99998a5c62&page=view&resid=375C2C99998A5C62!2705&parId=375C2C99998A5C62!2703&authkey=!AHH10BbZMBrqM0k&app=OneNote
- Respiratory:
>Embryology:
http://epomedicine.com/medical-students/lung-development-embryology-made-easy/
>Physio:
+/- curves from BRS physio
>Pathology:
Pathoma
==============================================
==============================================
General advices/Before Exam:
-Mnemonics:
Mnemonics (memory aids) are a very vital part of step 1 ( at least for me :D ) that make remembering stuff much easier. A lot of the data is very dry but it stuck to your mind with mnemonics especially with pictures. I suggest checking the mnemonics in First Aid itself, First Aid proposed errata and these two very awesome websites:
http://www.medicowesome.com
(for sure :D you ll find mnemonics for everything here)
https://mynotes4usmle.tumblr.com
-Concepts:
Although memorizing is very important for step1, be sure to understand the concept before memorizing it. This is especially true in physiology because one fact may be asked in many ways.
-How much time needed?
I have seen ppl doing it in a period as short as 5 months ( esp if step2 is done before) up to more than 1 year with others. In my case, It was on and off but if you want to put a timeline I would say 6-7 months.
-How many times do I have to do First Aid?
No fixed answer to this question. It depends on your type of studying. Are you the type who likes to read fast then revise again and again? Or you like one solid 1st time then a fast revision?
I personally prefer a very solid 1st studying time with mnemonics and concepts and a fast revision after that. In my case, I studied First Aid once and skimmed it once
-Active studying
After you study First Aid and solve Uworld, try asking First Aid facts in a question form, do that on Facebook groups,Whatsapp..or with your study partner. Asking facts in question form will let you see many lines in First Aid that your eyes can oversee!
-Every single line can be a question
Please don’t omit any line, diagram..curve in First Aid, anything can be asked!
-Arrangement
It is not necessary to study the subjects in a system exactly like First Aid
The 2 that are very connected are physiology and pathology. I sometimes used to finish Anatomy, Embryology and Pharmacology then go back to physiology and pathology.
-Taking notes
This really differs for every person, some ppl like to write notes on extra notebooks, others write on First Aid or add sticky notes to it.
I starting adding notes from Uworld to First Aid then I stopped and continued taking notes using the flashcard program/app: Anki
It lets you search, add pics, audio and video
Always remember the best notes are those you make yourself.
(Taking notes may take a lot of time sometimes so it’s ok too if you use other ppl notes)
-Revision
You can come up with any personalized revision schedule you like, for me, revision was done after I finish the whole chapter in addition to its Uworld questions in the form of questions and answers with my friends on Facebook/Whatsapp.
Some already made Anki decks are there for step1, the most famous one is the Bronsenchephalon deck.
-What if I need more?
I suggest making Google images and Youtube videos your new friend, they can simplify a lot of concepts. I didn’t use DIT videos so I can’t comment on them. Idea is when you need extra clarification go to youtube or google and don't feel obliged to watch video series like DIT or Kaplan..etc
I believe that watching Dr. Najeeb’s videos or studying Goljan or textbooks..etc is NOT needed and is beyond the scope of Step1 and will just take extra time from you with no much difference in score!
-Uworld..how many times?
Regardless of how many times you ll do it, the 1st time should be always so solid, understanding concepts, writing notes..etc
Because when you solve Uworld again, recall bias would kick in and you ll be able to answer some questions not because you understand them but because you remember the question.
-Uworld timed or not?
Many factors affect this, but if it is your first time with the USMLEs, you can do some blocks untimed in tutor mode then try timed mode, if you feel there is no problem with time, you can continue doing tutor mode.
Another method done by some ppl is to do Uworld tutor mode first read then timed mode in their 2nd read.
This is also affected by how fast you read English, how you train your eyes to omit distractors and by resisting the urge to re-reading the question sometimes.
With time, this becomes easier!
-Uworld system-wise, Subject-wise or mixed?
It depends on each person and each has his own approach.
I think the 1st time should be done system wise excluding anatomy, microbiology, biostat. Biochem and genetics
Eg: Cardio => physio, patholo, pathophsyio, pharm...same for other systems
Anatomy should be done all together, same for biochem, genetics, biostat, micro
This will help integrating the relevant data together.
Mixed mode can be done for marked questions or the 2nd read of Uworld ( depending on how many times you ll do Uworld)
-How to approach questions?
Always read the last line first...sometimes you may be asked a pharmacology question that is 10 lines long, then the question may be: the drug works by the following mechanism! This will greatly help in saving time for more questions in the exam.
After reading the last line, you can start reading the question from the start, a good thing is to highlight the abnormalities or the main points so your eyes can pinpoint what the question is asking.
-Kaplan Videos and qbank
This questions depends on your level. I did my step 1 after graduation and I did CK before that, so in my case, I felt I didn’t need videos to explain the basics for me.
>I felt kaplan videos were needed for biochem, because in First Aid biochem is not that clear.
My advice is to watch the videos by Dr. Sam Turco, then look at Kaplan Biochem book to read what he explained but don’t see other pages that he doesn’t talk about because they are low yield.
>Kaplan pharmacology vid by Dr. Raymond may be used to explain the general pharmacology part of inhibitors.
>Kaplan qbank: in my opinion, it is not needed but it may be used for more practice for genetics and biostats questions.
-Ethics!
Even after studying First Aid, Uworld, Conrad Fischer 100 ethics cases, you may find some questions in the exam in which you are left with 2 answers to choose from. Follow your guts and move on :D
-NBMEs
>My advice is doing NBMEs starting from NBME 15 ...till 19
At least do 2 NBMEs online to get used to the exam preferably NBME 18 and 19
In my opinion. Older NBMEs don't represent exam trend and may have some very strange questions..but if you have time, do the biostat, genetic bands questions to be more used to deal with those. If you really have more time and you want to do all of NBMEs, you can do them too but know the concepts.
>Take NBMEs as an average, mostly your score will be somewhere between your lowest and highest score, It is something good to see you score increasing in each NBME, but put in mind that mostly NBME17 is underpredictive and that online ones are graded differently than offline ones.
>If you get scores in NBMEs that are near the passing score postpone your exam till you get a satisfactory result! Step 1 score will haunt you all the way :D so give it your best shot :D
- Step 2 and Step 1
I did CK before Step 1 so it helped in Pathology, micro, ethics, biostat, behavioral and a lot of pharm. In short, any step that you do before will help in the next one which leads to shorter studying time.
Exam day:
-Sleep well..arrive early,,skip the tutorial
-Breaks during exam?
>If you skip the 15-min tutorial at the start of the exam, you ll have an hour of break time
>I took a break after each block with a larger break after my 3rd block, relaxing more, eating a bit more.
>Eat a bit in breaks, go to the restroom and try to relax your mind,
>Wear something that has less pockets to save time because you will be checked each time you enter the exam room after any break.
>Do a simulation test for yourself before the exam, spend 8 hours with breaks in between and know when you feel more tired or more hungry and decide how to divide breaks in the actual exam accordingly.
-WTF questions
No matter how much you study, be prepared to find some strange questions in the exam, don’t panic, just follow your common sense, choose an answer and go on.
After the exam:
>You ll feel some relief, you did a great job...8 hours are gone and It’s time to breaaathe and maybe eat a large meal :D
>Now your mind will start remembering every single stupid mistake you did and you ll feel like: Who did I do that????
>Now 2 things: either leave it and suppress your ideas and hide anything related to Step 1 or go and do a brainstorming session and remember everything to reach a level of internal peace with what you did.
>You ll have some waves of anxiety for score anticipation in the 3 weeks after your exam :D this is NORMAL :)
Good luck everyone!
Written by: Murad
Monday, March 12, 2018
Adverse reactions of Digitalis mnemonic
Hey guys
I am back :D
I am back :D
My first blog post of the year - Adverse effects of Digitalis ( Digitalis toxicity ) mnemonics
Though the ADRs are divided into extra-cardiac and cardiac symptoms, I will present a more systematic mnemonification ;p
Sunday, March 11, 2018
Pulp Stones
This post is about age changes in the pulp. If the first thing that comes to your mind is pulp stone! That's correct! So, Let's dive into pulp and learn more about it :))
In Pulp cavity, age changes causes
In Pulp cavity, age changes causes
- Cellular changes
- Fibrosis of tissue
- Pulp stones or denticles
- Diffuse calcification
Cellular changes
There is a decrease in
- Number of cells
- Size of cell
- Number of Organelles
Fibrosis of tissue
- Accumulation of bundles of fibers
- In radicular pulp: longitudinal fiber bundle
- In coronal pulp: diffuse fibers
Therefore collagen fiber content increases in pulp organ.
Pulp stone or denticle
- They are nodular or calcified masses
- They have calcium:phosphate ratio comparable to dentin
- They can be Single or multiple
- Present in functional and unerupted teeth
- It is present in both coronal and pulpal portion
Classification: According to structure
True pulp stone
- Rare
- Found in the apex region
- The remnant of epithelial root sheath within pulp induce pulp cells to differentiate into odontoblast to form dentin masses
False pulp stone: they appear as concentrically years of mineralized tissue
Classification: According to location
- Free pulp stone is entirely surrounded by Dentin
- Attached pulpstone is partially fused with Dentin
- Embedded pulpstone is entirely surrounded by pulp

This Post is written by Anisha Valli,
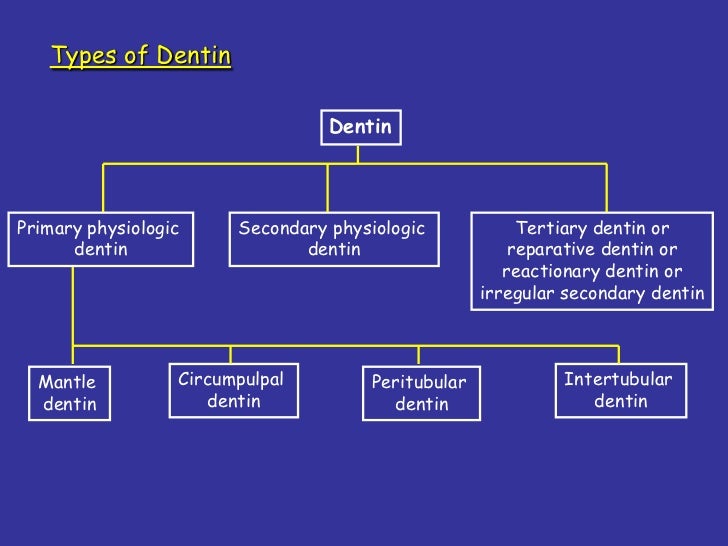
Types of Dentin
Hey friends,
Dentin is a very important question.
It comes as a question worth 4 points in my theory exam paper! I have tried my best to make it simpler for you all in this blog :))
I hope this will help you!
A. Mantle Dentin
Abrasion
Erosion
Cavity preparation
Written by Anisha Valli :))))
Primary Dentin
It is divided into Mantle and Circumpulpal Dentin
A. Mantle Dentin
- First formed dentin in the Crown
- Type III collagen
- It is less mineralized
- Matrix vesicles are present which help in Globular calcification
- It forms the bulk of the tooth
- Type one collagen
- It is more mineralized
- Matrix vesicles are present which help in Linear and globular calcification
Secondary Dentin
- It is formed after the root completion
- It contains dentinal tubules which are S-shaped
- The mineral ratio is similar to primary Dentin
- Secondary Dentin is a narrow band of Dentin bordering the pulp
- As age increases, inorganic content increases
- Therefore the Dentin becomes sclerosed
- It means It protects the pulp from exposure in older teeth
Tertiary Dentin
It is formed in response to stimuli
AttritionAbrasion
Erosion
Cavity preparation
- It is deposited on the pulpal surface of Dentin only in the affected area
- The appearance of Dentin varies as it is formed by an odontoblast
- Quality and quantity of tertiary Dentin depends on intensity and duration of stimuli
Reactionary Dentin
Dentin is deposited by pre-existing odontoblasts
Reparative Dentin
Dentin is deposited by newly differentiated odontoblast-like cellsWritten by Anisha Valli :))))
Friday, March 9, 2018
Understanding randomization in clinical trials
Hi,
I am writing this to clear basics about randomization. It is a very important concept for understanding the clinical trial design and can come handy while critically analyzing any trial or designing your own study.
This is not very important for any med school exam. I believe this is really important because of more extensive use of evidence-based medicine (EBM) in clinical practice and many clinicians lack the ability to skillfully evaluate a scientific manuscript.
I am planning to write more blogs related to evidence-based medicine, which might help our readers across the world to become expert in EBM.
Two most important features of successful randomization:
1. Procedure truly allocates treatments randomly (based on chance)
2. Assignments are tamper proof
Randomization techniques:
1. Simple randomization:
By coin flipping (one side for treatment 1 and another side for treatment 2), shuffled deck of cards (even numbers for treatment 1 and odd numbers for treatment 2), throwing dice (numbers <3 for treatment 1 and numbers >3 for treatment 2). More better methods are random table method in stats books and computer software like excel.
Uses: in large sample size (>100 it should be preferred over block randomization)
Drawback: problematic in small sample size because it can create unequal numbers in groups.
2. Block randomization: Ensure that participants are equally distributed among each group. Randomization is done in blocks, eg block size of six.
For example, a scientist enrolls only 6 patients per visit for a trial of total 60 patients. On each visit, he divides 3 patients each to treatment group A and B. At the end he will have 30 patient in both groups. See the figure 1 below.

Figure 1. Block randomization of 60 patients in 6 patient blocks.
Drawbacks: Not suitable for randomization in non blinded trials, because randomization in small blocks makes a prediction of sequence easy.
3. Stratified Block randomization: It ensure that important predictor of outcome is more evenly distributed among study groups.
For example, if the age is a major determining factor in effectiveness or toxicity of the treatment then its imperative to have a similar distribution of ages in both treatment groups. Hence patients will be the first stratified into age groups and then they will be equally randomized in each arm. Like we did for Block randomization.
Drawback: only small number of baseline variables (2-3) can be managed by this technique.
4. Adaptive randomization: used for balancing more than 2-3 baseline variables.
5. Minimization: more complex adaptive randomization
I will continue more in next blog on randomization or other important concepts. Kindly post comments or question, which might help me, you, or other readers.
Thanks,
Dr. Gee
References:
Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Designing clinical research. Lippincott Williams & Wilkins; 2013 May 8.
Suresh, K. (2011). An overview of randomization techniques: An unbiased assessment of outcome in clinical research. Journal of Human Reproductive Sciences, 4(1), 8–11. http://doi.org/10.4103/0974-1208.82352
I am planning to write more blogs related to evidence-based medicine, which might help our readers across the world to become expert in EBM.
- RANDOMIZATION - randomly allocating participants into different treatment arms, purely on the basis of chance.
- Randomization is the cornerstone of clinical trial design. It's a very tricky concept and gets trickier when you start evaluating scientific literature critically or start designing a robust clinical trial.
- It is pivotal in distributing confounders (eg. sex, age, history) equally in every treatment arm. Except for chance variation among the randomized group at baseline
Two most important features of successful randomization:
1. Procedure truly allocates treatments randomly (based on chance)
2. Assignments are tamper proof
Randomization techniques:
1. Simple randomization:
By coin flipping (one side for treatment 1 and another side for treatment 2), shuffled deck of cards (even numbers for treatment 1 and odd numbers for treatment 2), throwing dice (numbers <3 for treatment 1 and numbers >3 for treatment 2). More better methods are random table method in stats books and computer software like excel.
Uses: in large sample size (>100 it should be preferred over block randomization)
Drawback: problematic in small sample size because it can create unequal numbers in groups.
2. Block randomization: Ensure that participants are equally distributed among each group. Randomization is done in blocks, eg block size of six.
For example, a scientist enrolls only 6 patients per visit for a trial of total 60 patients. On each visit, he divides 3 patients each to treatment group A and B. At the end he will have 30 patient in both groups. See the figure 1 below.

Figure 1. Block randomization of 60 patients in 6 patient blocks.
Drawbacks: Not suitable for randomization in non blinded trials, because randomization in small blocks makes a prediction of sequence easy.
3. Stratified Block randomization: It ensure that important predictor of outcome is more evenly distributed among study groups.
For example, if the age is a major determining factor in effectiveness or toxicity of the treatment then its imperative to have a similar distribution of ages in both treatment groups. Hence patients will be the first stratified into age groups and then they will be equally randomized in each arm. Like we did for Block randomization.
Drawback: only small number of baseline variables (2-3) can be managed by this technique.
4. Adaptive randomization: used for balancing more than 2-3 baseline variables.
5. Minimization: more complex adaptive randomization
I will continue more in next blog on randomization or other important concepts. Kindly post comments or question, which might help me, you, or other readers.
Thanks,
Dr. Gee
References:
Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Designing clinical research. Lippincott Williams & Wilkins; 2013 May 8.
Suresh, K. (2011). An overview of randomization techniques: An unbiased assessment of outcome in clinical research. Journal of Human Reproductive Sciences, 4(1), 8–11. http://doi.org/10.4103/0974-1208.82352
Wednesday, March 7, 2018
Management of Stroke
Hello, seeker of knowledge! Let’s see how we manage one the most common emergencies in medicine, stroke or cerebrovascular accident.
PRE-HOSPITAL CARE:
Cincinnati Pre-Hospital Stroke Scale (CPSS) helps make a prompt diagnosis and includes FAST -
Face drooping
Arm weakness
Speech difficulty
Time to call Emergency Medical Services
HOSPITAL CARE:

TIA = Transient Ischemic Attack
ABC = Airway, Breathing and Circulation
BGL = Blood Glucose Level; Both HYPO- and HYPER- glycemia are to be corrected
Hhg = Hemorrhage
Lytes=Electrolytes; ABG =Arterial Blood Gas; RFT=Renal Function Test; LFT=Liver Function Test
rTPA = recombinant tissue plasminogen activator
ASA = Acetyl Salicylic Acid = Aspirin
UFH = Unfractionated Heparin; LMWH = Low Molecular Weight Heparin
ADDITIONAL INVESTIGATIONS MAY BE DONE - PROVIDED THROMBOLYSIS, IF INDICATED PER CT - IS NOT DELAYED
TREATMENT PRINCIPLES:
To minimize:
Ischemic penumbra (area around umbra/ ischemia)
Secondary brain injury
Risk of recurrence
THROMBOLYSIS:
INDICATIONS -
Mnemonic: ADD 1/3rd to CT after consent
Age 18 years or more
Diagnosis of Acute Ischemic Stroke(AIS)
Duration of symptoms 4.5 hours or less
AIS involves more than 1/3rd MCA territory
CT reveals no hemorrhage or edema
Consent of the patient or surrogate decision maker
CONTRAINDICATIONS -
Mnemonic: SHIP BLAST
Stroke in the last 3 months
Head injury in last 3 months
Intracranial hemorrhage
Prothrombin Time > 15 sec
BP > 185/110
Lumbar puncture in last 7 days
Anticoagulants use / Arterial puncture in last 7 days
Surgery within last 14 days
Thrombocytopenia < 100,000
PRECAUTIONS:
No anti-thrombotics for 24 hours
No Foley’s catheter for 2 hours
ADVERSE DRUG REACTIONS:
Intra-cranial hemorrhage
Allergy
ANTI-COAGULANTS:
INDICATIONS:
Mnemonic: My L.A.P.D. job
Recent MI
Left ventricle aneurysm or dyskinesia
Atrial fibrillation
Prosthetic heart valve
Deep vein thrombosis prophylaxis
MEDICINE PEARL: MI and stroke have essentially the same pathophysiology. Clots blocking arteries! However, we give DUAL anti-platelet therapy [DAPT], i.e. Aspirin and Clopidogrel for MI while there’s only Aspirin administered to a patient with stroke.
NURSING CARE:
Bowel and bladder care
Prevention and treatment of bed sores
REHABILITATION:
Use of walkers and crutches
Full range of active and passive joint movements
FURTHER READING:
Other rehabilitative therapies offered
Risk factors and preventive strategies
Alternative drugs and procedures
Hope this helps. Happy studying!
-- Ashish Singh.
PRE-HOSPITAL CARE:
Cincinnati Pre-Hospital Stroke Scale (CPSS) helps make a prompt diagnosis and includes FAST -
Face drooping
Arm weakness
Speech difficulty
Time to call Emergency Medical Services
HOSPITAL CARE:

TIA = Transient Ischemic Attack
ABC = Airway, Breathing and Circulation
BGL = Blood Glucose Level; Both HYPO- and HYPER- glycemia are to be corrected
Hhg = Hemorrhage
Lytes=Electrolytes; ABG =Arterial Blood Gas; RFT=Renal Function Test; LFT=Liver Function Test
rTPA = recombinant tissue plasminogen activator
ASA = Acetyl Salicylic Acid = Aspirin
UFH = Unfractionated Heparin; LMWH = Low Molecular Weight Heparin
ADDITIONAL INVESTIGATIONS MAY BE DONE - PROVIDED THROMBOLYSIS, IF INDICATED PER CT - IS NOT DELAYED
TREATMENT PRINCIPLES:
To minimize:
Ischemic penumbra (area around umbra/ ischemia)
Secondary brain injury
Risk of recurrence
THROMBOLYSIS:
INDICATIONS -
Mnemonic: ADD 1/3rd to CT after consent
Age 18 years or more
Diagnosis of Acute Ischemic Stroke(AIS)
Duration of symptoms 4.5 hours or less
AIS involves more than 1/3rd MCA territory
CT reveals no hemorrhage or edema
Consent of the patient or surrogate decision maker
CONTRAINDICATIONS -
Mnemonic: SHIP BLAST
Stroke in the last 3 months
Head injury in last 3 months
Intracranial hemorrhage
Prothrombin Time > 15 sec
BP > 185/110
Lumbar puncture in last 7 days
Anticoagulants use / Arterial puncture in last 7 days
Surgery within last 14 days
Thrombocytopenia < 100,000
PRECAUTIONS:
No anti-thrombotics for 24 hours
No Foley’s catheter for 2 hours
ADVERSE DRUG REACTIONS:
Intra-cranial hemorrhage
Allergy
ANTI-COAGULANTS:
INDICATIONS:
Mnemonic: My L.A.P.D. job
Recent MI
Left ventricle aneurysm or dyskinesia
Atrial fibrillation
Prosthetic heart valve
Deep vein thrombosis prophylaxis
MEDICINE PEARL: MI and stroke have essentially the same pathophysiology. Clots blocking arteries! However, we give DUAL anti-platelet therapy [DAPT], i.e. Aspirin and Clopidogrel for MI while there’s only Aspirin administered to a patient with stroke.
NURSING CARE:
Bowel and bladder care
Prevention and treatment of bed sores
REHABILITATION:
Use of walkers and crutches
Full range of active and passive joint movements
FURTHER READING:
Other rehabilitative therapies offered
Risk factors and preventive strategies
Alternative drugs and procedures
Hope this helps. Happy studying!
-- Ashish Singh.
Subscribe to:
Posts (Atom)