
Injection Techniques

INTRAMUSCULAR INJECTION

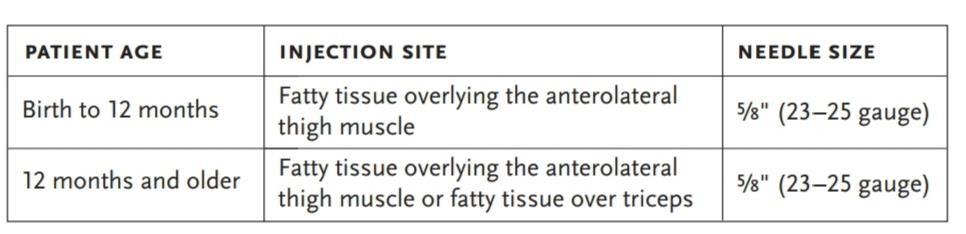
Preferred Site:
0-2 years: Anterolateral thigh
3 years old and above: Deltoid
(In children ages less than 15 months the deltoid muscle is not safe to use since it is not developed enough to absorb the vaccine and the radial nerve is close to the surface)
REQUIREMENTS:
Cotton, Antiseptic, 22-25 G needle, Syringe
PROCEDURE:
Child should be in mothers lap and mother holding hands of infant


ADMINISTRATION:
Use aseptic precautions
Hold the syringe barrel with fingers and thumb on sides of the barrel and with the bevel (hole) of the needle facing upwards
Pinch and gather the muscle mass by one hand
Stretch the skin over injection site
Insert needle at 90 degree
Aspirate to make sure a blood vessel is not punctured. DO NOT ASPIRATE WHEN YOU INSERT THE NEEDLE INTO THE INFANT FOR THE INJECTION.
Depress the plunger smoothly, taking care not to move the needle under the skin
Pull the needle out quickly and smoothly at the same angle as it went in
Place a clean swab gently over the site
DO NOT RUB OR MASSAGE the injection site. Soothe and distract the infant
Discard everything according to biomedical waste rules
Dosage of Anti-Rabies Serum: 20 IU/kg, half at bite site and half intra-muscularly
SUBCUTANEOUS INJECTION
The injection is given into the layer below the skin on the upper arm
REQUIREMENTS:
Cotton, Antiseptic, 22-25 G needle, Syringe
PROCEDURE:
POSITION:
Child should be in mothers lap and mother holding hands of child and exposing upper arm of baby


ADMINISTRATION:
Wash hand and wear sterile gloves
Hold the syringe barrel with fingers and thumb on the sides of the barrel and with the bevel (hole) of the needle facing upwards
Quickly push the needle into pinched up skin at a 45degree angle
Direct it towards the shoulder of the child
Depress the plunger smoothly, taking care not to move the needle under the skin
DO NOT RUB OR MASSAGE the injection site. Soothe and distract the infant
Pull the needle out quickly and smoothly at the same angle as it went in
Place a clean swab gently over the site
Discard everything according to biomedical waste rules
INTRADERMAL INJECTION
BCG is the only vaccine that is injected intradermally (into the layers of the skin) for slow absorption. It is usually given in the left upper arm. To measure and inject the very small dose (0.05 ml) accurately, a special syringe and needle are used.
POSITION:
Cuddle position on caregiver’s lap (BCG recommended for infants only)

ADMINSTRATION:
Hold the syringe barrel with fingers and thumb on the sides of the barrel and with the bevel (hole) of the needle facing upwards
Lay the syringe and needle almost flat along the infant’s skin
Insert the tip of the needle under the surface of the skin just past the bevel
Keep the needle close to the skin at the same angle as you inserted it
Place your other thumb on the lower end of the syringe near the needle to hold the needle in position, but do not touch the needle.
Hold the plunger end of the syringe between the index and middle fingers. Press the plunger in slowly with the thumb. If you feel no resistance to the plunger, you are not in the right place and should reposition
A pale flat-topped swelling with small pits like an orange peel should appear on the skin
Remove the needle smoothly at the same angle as it went in
The caregiver should place a clean swab gently over the site
DO NOT RUB OR MASSAGE the injection site. Soothe and distract the infant
Discard everything according to biomedical waste rules
REFERENCES:
http://www.who.int/immunization/policy/Immunization_routine_table2.pdf? ua=1

















