
Friday, August 18, 2017

Drug of choice : Dermatology
Hello everyone!
Here's a collection of Drugs of choice (DOC) for some Dermatology conditions. These are some of the most commonly asked questions in Post Graduation entrance exams.
1. DOC for severe erythrodermic psoriasis?
Cyclosporin
2. DOC for erythrodermic psoriasis?Methotrexate
3. DOC for pustular psoriasis?
Acitretin
4. 2nd choice for pustular psoriasis?Methotrexate
5. DOC for arthritis mutilans?
Etanercept
6. DOC for impetigo herpetiformis?
Systemic steroids
7. DOC for psoriatic arthritis?
Methotrexate
8. DOC for psoriatic erythroderma in pregnancy?
Systemic steroid
-Md Mobarak Hussain (Maahii)
Thursday, August 17, 2017
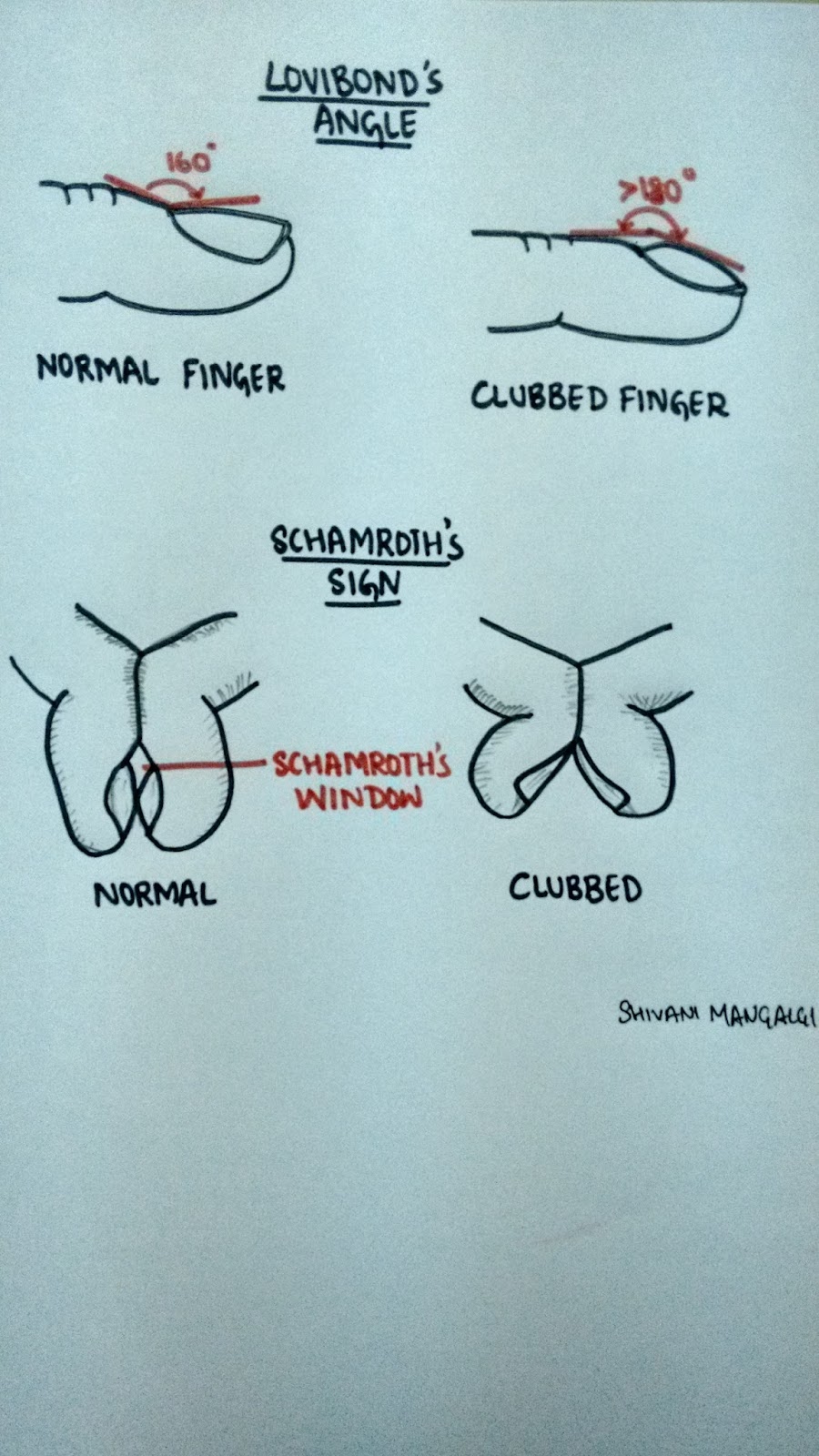
Clubbing
Bulbous enlargement of the distal portion of the digits due to increased subungual soft tissue.
It is also known as the "Hippocratic fingers", as it is believed that perhaps Hippocrates was the first to document clubbing as a sign of disease.
Grades of clubbing-
Grade I- presence of fluctuation test °
Grade II- obliteration of Lovibond angle*
Grade III- parrot beak or drumstick appearance
Grade IV- hypertrophic osteoarthropathy (HOA)
*Refer the diagram
°Refer the video clipping
Theories of clubbing-
1. Neurogenic theory- vagal stimulation via neural reflexes can lead to proliferation of connective tissue at the distal extremities resulting in clubbing.
2.Humoral theory- Normally lungs throws out all the soluble substances by inactivation. But in case of lung problems, these systems reach the systemic circulation in active state and stimulate the changes seen in HOA (growth hormone, PTH, bradikynin, prostaglandin, ferritin)
3.Hypoxic theory- Hypoxia is suggested to be a stimulus for HOA. It leads to opening of deep arteriovenous shunts and fistulae which increase blood flow to the extremities and leads to hypertrophy.
4.Platelets derived growth factor- Normally megakaryocytes and large platelets get destroyed in the lungs. But in lung pathology they escape the lung and reach the distal extremities. Here they interact with the endothelial cells and release platelet derives growth factor (PDGF) post activation. PDGF and other mediators then activate the fibroblasts and transforming growth factor beta which lead to collagen production and connective tissue laying down ultimately giving rise to clubbing and HOA.
This is the latest accepted theory.
Causes of clubbing-
'CLUBBING'
C - cyanotic heart diseases, chron's disease
L - lung causes (lung abscess, emphysema, interstitial lung disease, bronchogenic carcinoma, tuberculosis)
U - ulcerative colitis
B - biliary cirrhosis
B - benign mesothelioma
I - infective endocarditis, idiopathic, inherited
N - neurogenic tumors
G - graves disease
Shivani Mangalgi
Medicowesome 2017
Hypergraphia - An intriguing brain anomaly
It is a condition in which an individual feels the driving compulsion to write; the overwhelming urge to write.
Hypergraphia has also been called 'midnight disease'.
Well based on how we perceive it, the "disease" could either be all about writing or writer's block.
Neurologically-
This unstoppable drive to write can be triggered by temporal lobe epilepsy(hippocampus and Wernicke's area in specific), intolerant mood disorders or dopamine.
What is very fascinating about this condition is that there are NO other vicious symptoms (other than a little irritability-which is quiet expected) and the fact that the patient can go on writing on anything from toilet papers to wall to even roads.
And what is more fascinating to know is that many famous authors and poets like Sylvia Plath, Stephen King and Leo Tolstoy (that's how the world got "War and Peace") suffered from hypergraphia.
Ingenious result from a brain defect.
Now a question might arise..if the quality of writing in these patients is any good?
To answer this, it is important to know that patient with hypergraphia exhibit wide variety of writing style and content. To elucidate this statement, let's go through few accounts:
1. Alice Flaherty (Harvard Medical school neurologist) gets episodes of hypergraphia following any grief incidences that have grave affect on her brain.
She has started her 4th book and is doing research to help explain how the muse comes and goes.
2. Mendez- He felt the unreasonable compulsion to write poetry even though the patient had no previous history of being a poet.
3. Patient who wrote everything backwards!
4. Patients writing same word over and over again but with differing calligraphy.
5. Patients' writing consists of sheer scribbling and frantic random thoughts.
Therefore on a lighter note, if you have the wrong brain defect but fall under the right category...then voilà...YOU shall be famous!
Shivani Mangalgi
Medicowesome 2017
Leucocoria
Also known as the white pupillary reflex, is an abnormal white reflection from the retina of the eye.
Pathologically it's the absence of the red reflex.
Clinically the pupils appear white rather than the usual black color.
Mnemonic for causes of leukocoria-
'CREAM PIGMENT'
C - Coats disease/ Coloboma/ Cataract
R - Retinoblastoma/ Retinal dysplasia/ ROP/ Retinal fold
E - Endophthalmitis
A - Astrocytic hamartoma/ Anisometropia
M - Myelinated retinal nerve fiber layer
P - Persistent fetal vasculature/ PHPV
I - Incontinentia pigmenti/ Inflammation (uveitis)
G - Granuloma
M - Melanoma/ Medulloepithelioma
E - Familial exudative vitreoretinopathy (FEVR)
N - Norrie
T - Trauma/ Toxocariasis
Go ahead and add more causes to make your own list!
Shivani Mangalgi
Medicowesome 2017
Post operative ileus ( mechanical obstruction vs paralytic )
- No return of bowel movements ( on auscultation ) after 72 hours
- Absence of flatus or stool on day 6 after surgery
- Feeling of discomfort, nausea or vomiting on oral intake, thus requiring i.v. support, NG tube placement by PO day 5.
- Partial return of bowel movements after PO day 5.
( Refer to UpToDate)
Hope this helps :)
Wednesday, August 16, 2017
Causative microbes in acute osteomyelitis
Hello Awesomites!
Let's discuss some facts about Common microbes involved in Acute Osteomyelitis.
Staphylococcus aureus is the most common infecting organism found in older children and adults with osteomyelitis.
Gram negative bacteria - vertebral body infections in adults.
Pseudomonas - intravenous drug abusers.
Fungal osteomyelitis - chronically ill patients receiving long-term intravenous therapy or parenteral nutrition.
Salmonella osteomyelitis - Sickle cell hemoglobinopathies - tends to be diaphyseal.
Infants -S. aureus (most common),group B streptococcus & gram-negative coliforms .
Group B streptococcus - otherwise healthy infants 2 to 4 weeks of age.
Animal Bite - Pasteurella
Human Bite - Eikinella
That's all!
Thank you.
MD Mobarak Hussain (Maahii)
Tuesday, August 15, 2017
Paramedian pontine reticular formation and MLF

-Upasana Y. :)

Third nerve palsy
Before starting with the III nerve, Let us understand the term.
According to TABER'S medical dictionary, We need to understand 3 main type of palsy here.
1.NUCLEAR palsy :- Paralysis caused by lesion of the nuclei in CNS.
2.OCULAR palsy :- Paralysis of extraocular nd intraocular muscles.
3.MUSCULAR palsy :- Loss of the capacity of muscle to contract. It may be due to structural or functional disorders
-in the muscle at the myoneural junction,
-in efferent nerve fibres,
-in the cell bodies of nuclei of origin of the brain or of the gray matter of the spinal cord,
-in conducting pathways of the brain or spinal cord,
-in motor centres of the brain.
Third cranial nerve supplies
1. EXTRAOCULAR MUSCLES
-Superior rectus
-Inferior oblique
-Medial rectus
-Inferior rectus
2.INTRAOCULAR MUSCLES
-Levator palpebral superioris
-Ciliary body
-Iris sphincter msucle
THE LOCALIZATION OF THIRD NERVE LESION
-Supranuclear
-Nuclear
-Fascicular
-Basilar
-Intra-Cavernous sinus
-Superior orbital fissure
-Intra Orbital part
CLINICAL FEATURES OF THIRD NERVE PALSY:-
1. Ptosis - paralysis of LPS muscle.
2. Deviation – out, down and intorted (unopposed action of LR and SO).
3. Ocular movements:
• Adduction – MR
• Elevation – SR and IO
• Depression – IR
• Extorsion – IR and IO
4. Pupil is fixed and dilated – paralysis of sphincter pupillae muscle.
5. Accommodation is completely lost – paralysis of ciliary muscle.
6. Crossed diplopia – paralytic divergent squint.
7. Head posture – If the pupillary area is uncovered, head takes a posture consistent with the directions of actions of the paralysed muscles, i.e., head is turned on the opposite side, tilted towards the same side and chin is slightly raised. (Pathways between vestibular nuclei and oculomotor nuclei. These are Intranuclear pathway.)
FEATURES AND CAUSES OF THIRD NERVE LESIONS AT VARIOUS LEVELS
1. Supranuclear lesions
• Lesions of the cerebral cortex and supranuclear pathway produce conjugate paresis which affect both eyes equally.
• In supranuclear lesions although position and movements of the eyes are abnormal, they maintain their relative co-ordination and produce no diplopia.
2. Nuclear lesions
• Lesions involving purely the third nerve nucleus are relatively uncommon.
• Common causes include ; vascular diseases, demyelination, primary tumors and metastasis
• Lesions involving entire nucleus cause
-an ipsilateral third nerve palsy with ipsilateral sparing and
-contralateral weakness of elevation.
• Lesions involving paired medial rectus subnuclei (ventromedial nucleus) cause a wall-eyed bilateral internuclear ophthalmoplegia ( WEBINO ) characterised by defective convergence and adduction.
-PULSATILE EXOPHTHALMOS can also be seen.
• Causes :
I want to thank my teacher for such a beautiful explanation.
I hope it helped.
Do read about the following . (though I will write on this topic also)
1.Injury of Paramedian pontine reticular formation
2. Ptosis in Horner's syndrome and oculomotor nerve palsy.
Drugs that can cause TOXIC MYOPATHIES
1. TYPE- Inflammatory
-Cimetidine
-D- Penicillamine
-Procainamide
-L-tryptophan
-Levodopa
2.TYPE- Non-Inflammatory necrotizing or vacuolar
-Alcohol
-Cholestrol lowering agents
-Chloroquine
-Colchicine
-Cyclosporine and tacrolimus
-Emetine
-Isoretinoic acid
-Vincristine
-Labetalol
3.TYPE -Rhabdomyolysis and myoglobinuria
-Alcohol
-Amphetamine
-Cocaine
-Heroin
-Phencyclidine
-Meperidine
4.TYPE -myosin loss
-Non depolarizing neuromuscular blocking agent
-steroid
That's all.
-Upasana Y. :)
Monday, August 14, 2017
ABC vs CAB for CPR
If someone ask the medical personnel, What is ABC ?
Unfailingly, the answer will be A-airway, B-breathing ,C-Circulation.
But now this has been changed to C-A-B.(I didn't know this)
C-Compression /circulation
A-airway
B-breathing
(SOURCE :- I took the following content from https://medictests.com/abc-vs-cab-correct/ )
In 2010 the AHA made a radical change to how we approach CPR. Up until then we all lived by the trusty "ABC" (Airway, Breathing, Circulation) method of resuscitation. Not surprisingly, though, the AHA's ongoing research began to show that compressions are the most important part of CPR and any delay or interruption resulted in worse outcomes. It was also discovered that during CPR, the patient's blood stays oxygenated for 4-6 minutes after their last breath. In response to this research, and in an attempt to simplify CPR for untrained laypeople, the AHA decided to switch our initial approach from ABC to CAB. While this change is medically sound, it has cause a lot of confusion for healthcare professionals who regularly use ABC for other scenarios. So, ABC vs CAB, which is correct?
With indisputable evidence that compressions are the most important part of CPR, it is no wonder that AHA has been dee-mphasizing airway and breathing. In fact, in ACLS, the AHA has gone as far as to suggest that endotracheal intubation may not be as important as we once thought. While it remains the ultimate airway, the AHA suggests BVM or supraglottic airway ventilations because they reduce the interruption of compressions.
In accordance with this paradigm shift, the AHA has changed ABC to CAB in the event of cardiac arrest. Unfortunately, though, some healthcare providers have incorrectly interpreted this change in cardiac arrest to be a change that applies to every other medical call. Some are under the impression that the AHA is the governing body over prehospital and emergency care, which is simply not the case. CAB is no doubt a revolution in cardiac arrest care but it is not meant to change the way we approach our "normal" patients.
Here is a short list of examples of when ABC vs CAB should be used
ABC
Overdose
Trauma
Altered mental status
Diabetic emergencies
Respiratory failure
Airway obstruction
Respiratory Distress
CAB
Cardiac Arrest
Conclusion:-
It does not have to be one or the other! While ABC has been phased out by the AHA, it still is the de facto initial assessment used in every non-cardiac arrest call. CAB, on the other hand, is now being used during cardiac arrest to remind practitioners and laypeople of the importance of compressions. In general, it is not useful to confine yourself to one ideology "because they say so." It is much more productive to understand each approach and use critical thinking to choose the best route for your patient.
That's all
-Upasana Y. :)
Saucerization and Arthrodesis
I was fascinated with this two terms :- Saucerization in Osteomyelitis and Arthrodesis (I studied it in treatment of foot drop).
SAUCERIZATION
-Extension of surgical debridement
-Debrided wounds left open widely through excision of overhanging soft tissue and bone
-Wounds drain freely (otherwise If we close it the pus will keep on collecting)
-Abscesses do not form
-Limited to areas where it causes acceptable loss of function e.g. Tibia and femur
Arthrodesis
The term arthrodesis refers to surgical fusion of a joint.
The indications for this are pain & instability in a joint and, in some situations, following the failure of joint replacement.
FIXATION POSITIONS
The optimum positions for arthrodesis in different joints are as follows:
1. SHOULDER:
-In such a position that the hand can comfortably reach the mouth.
-The person will be able to perform the day-to-day activity like eating.combing,scratching the back,cleaning.
-Arthrodesis of shoulder joint is usually reserved for a flail joint as may follow a brachial plexus injury.
-Stabilization of this joint may lead to improvement in the remaining distal function of the arm.
2. ELBOW: 90° of flexion.
(Suppose you won't be able to flex it 90 degree ,then what will happen? Try eating food with that position. You won't be able to do that without this.)
3. WRIST: A few degree of extension
4. THUMB:
-MCP joint in 20° of flexion.
-IP joint in slight flexion.
5.FINGERS:
MCP joints in 20° -30° of flexion.
(These joints are rarely fused).
Proximal IP joints in 40° -45° of flexion (less in middle & index fingers)

Casts (Colle's Cast)
These days, I am attending orthopaedics posting. And I am loving it.
I saw casting. Following questions were asked to me during the procedure.
Q. Define Casts and Slabs.
A. Cast & slab are methods of a temporary immobilization for a wide variety of musculoskeletal conditions not only for disorders of bones but also for many other disorders related with tendons, muscles and soft tissues
Cast: are circumferential immobilizers which is surrounding the whole circumference of the limb
Slab: are non-circumferential immobilizers which is only support apart of the circumference of the limb.
Q. Define Traction and Splints.
A. TRACTION -Traction is a method of restoring alignment to a fracture through gradual neutralisation of muscular forces. Traction is applied to the limb distal to the fracture, so as to exert a continuous pull in the long axis of the bone.
SPLINT - A device used for support or immobilization of a limb or the spine. Any material used to support a fracture is known as splint.
Q. What is Colle's Fracture?
A. It is not just fracture lower end of radius but a fracture dislocation of the inferior radioulnar joint.
Q. Do you know anything regarding Colles Cast.
A. It is a type of Immobilization method. It is the Below elbow cast (10 – 20 degree palmar flexion, 15 – 20 degree ulnar deviation) .
So, Colle`s cast :- It is a below elbow cast in supination.
Ideally it has to meet the following 4 criteria :
-Firm fit at the dorsum
-Firm fit at the volar fracture apex
-Just snuggly fitting at the forearm
-Metacarpophalangeal joints should be free to move.
Arsenic Poisoning
Hello awesomites!
Here's a Mnemonic on Arsenic Poisoning
The mnemonic is AR4SENIC
A-Aldrich Mees line (Nail)
R-Raindrop pigmentation
Reinsch Test (Gutzeit test used nowadays)
Rashes(fading measles rashes)
Red velvety mucosa(Postmortem finding)
S-Subendocardial hemorrhage(Postmortem finding)
E-Excess pigmentation and keratosis (Palms and soles)
N-Neuritis
I-Iron oxide n BAL(antidote)
C-Cholera like symptoms
I hope that it's helpful.
That's all!
Thank you.
Diagnostic criteria of neurofibromatosis type 1 mnemonic
The criteria are met in an individual if two or more of the features listed are present.
The mnemonic is "FANCOOL"
F: Family history
A: Axillary freckles (known as CROWE'S SIGN)
N: Neurofibromas (2 or more)
C: Café-au-lait macules (6 or more)
O: Optic gliomas
O: Osseous (sphenoid dysplasia)
L: Lisch nodules in the eyes.
Thanks for reading.
Madhuri
Sunday, August 13, 2017
Diagnostic features in the X-ray and probable pathology in the Sinus
1. Haziness of sinuses only :- Sinusitis
2. Bony expansion without erosion :- Benign tumefaction e.g Polyposis
3. Decreased air shadow in nasal cavity without bony expansion :- Hypertrophic rhinitis
4. Bony erosion with expansion :- Malignancy
5. Bony defect without expansion of haziness :- Surgically induced (Iatrogenic) or fracture
6. Fluid level in maxillary sinus :- Sinusitis with pus signifying acute bacterial maxillary sinusitis
This question was asked to me by my friend and it was fun to find the answer.
(Source :-Otolaryngology at the eleventh hour By Anupam Mishra)
That's all for today.
-Upasana Y. :)
Saturday, August 12, 2017
New treatment regimen for Hepatitis C
Hey guys! I have copied this article from the FDA website more or less. You will definitely find it helpful.
The U.S. Food and Drug Administration today approved Mavyret (glecaprevir and pibrentasvir) to treat adults with chronic hepatitis C virus (HCV) genotypes 1-6 without cirrhosis (liver disease) or with mild cirrhosis, including patients with moderate to severe kidney disease and those who are on dialysis. Mavyret is also approved for adult patients with HCV genotype 1 infection who have been previously treated with a regimen either containing an NS5A inhibitor or an NS3/4A protease inhibitor but not both.
Mavyret is the first treatment of eight weeks duration approved for all HCV genotypes 1-6 in adult patients without cirrhosis who have not been previously treated. Standard treatment length was previously 12 weeks or more.
“This approval provides a shorter treatment duration for many patients, and also a treatment option for certain patients with genotype 1 infection, the most common HCV genotype in the United States, who were not successfully treated with other direct-acting antiviral treatments in the past,” said Edward Cox, M.D., director of the Office of Antimicrobial Products in the FDA’s Center for Drug Evaluation and Research.
There are at least six distinct HCV genotypes, or strains, which are genetically distinct groups of the virus. Knowing the strain of the virus can help inform treatment recommendations.
The safety and efficacy of Mavyret were evaluated during clinical trials enrolling approximately 2,300 adults with genotype 1, 2, 3, 4, 5 or 6 HCV infection without cirrhosis or with mild cirrhosis. Results of the trials demonstrated that 92-100 percent of patients who received Mavyret for eight, 12 or 16 weeks duration had no virus detected in the blood 12 weeks after finishing treatment, suggesting that patients’ infection had been cured.
Treatment duration with Mavyret differs depending on treatment history, viral genotype, and cirrhosis status.
The most common adverse reactions in patients taking Mavyret were headache, fatigue and nausea.
Mavyret is not recommended in patients with moderate cirrhosis and contraindicated in patients with severe cirrhosis. It is also contraindicated in patients taking the drugs atazanavir and rifampin.
That's all!
-VM