Since the bulk assign option isn't available before 15th September:

Thursday, September 14, 2017
Sunday, September 10, 2017
Enucleation, Evisceration & Exenteration
In this post, we will look at the definition, indications and some few details regarding these 3 ophthalmologic surgeries.
Saturday, September 9, 2017
Cytochrome P450 3A4
Hello everyone!
Today lets discuss the Cytochrome P450 3A4
It is the microsomal enzyme involved in metabolism of xenobiotics. Maximum number of drugs are metabolised by CYP 3A4 in our body.
Here’s how you remember the substrates and the inducers of the enzyme:
“In emergency Straightaway give a CPR and ACT SaNely
The inducers are:
S: St John Wort
CPR: Carbamazepine, Phenytoin, Phenobarbitone, Rifampicin
The substrates are:
ACT SaNely
A-Amiodarone
A-ACT drugs(Anti Histamines)
*A-Astemizole
*C-Cisapride
*C-Cisapride
*T-Terfenadine
C- Cyclosporine
T- Tacrolimus
S- Statins
N-Navirs (protease inhibitors)
N-Navirs (protease inhibitors)
And how do we remember the inhibitors?
Shout “Fire in the Hole!”
Fluconazole Ketoconazole
and Ritonavir and Erythromycin
Also you can have some grapefruit juice to chill out! Grapefruit juice is also a Inhibitor of CYP3A4.
That’s all
Thank you,
Chaitanya Inge
Tuesday, September 5, 2017
Drug interaction
Hello :)
Definition:-
Modification of response to one drug by another drug or non drug (like food ,beverages like alcohol,smoking) when they are administered simultaneously or in quick succession .
Factors for drug interactions:-
1.Multiple drugs for same disease.
2.Multiple prescribers.
3.Multiple diseases.
4.Poor patient compliance .
5. Drug factors like it is not palatable or too many in frequency .
6.Multiple unknown action of drugs.
7. Most imp is patients age .
Effects of drug interaction:-
1.Quantitative i.e Increase or decrease the response intensity.
2. Qualitative:- abnormal /different type of response.
Mechanism of drug interaction :-
A.Pharmacokinetic interactions include,
1.Absorption (either complex formation ,pH change ,or alteration in motility of GIT.)
2. Distribution:- (displacement from plasma protein binding site + inhibition of metabolism /or excretion)
3. Metabolism:- ( induction of enzymes or inhibition of enzymes or hepatic blood flow)
4.Excretion:- ( alteration in urine pH, Competition for active secretion ,renal blood flow)
B. Pharmacodynamic drug interactions include,
1.Antagonism
2. Summation
3.synergism
C.Drug interaction before administration:-
Either mixing before administration.
Or, exposure to light in some cases. (Like sodium nitroprusside).
-Upasana Y.
Definition:-
Modification of response to one drug by another drug or non drug (like food ,beverages like alcohol,smoking) when they are administered simultaneously or in quick succession .
Factors for drug interactions:-
1.Multiple drugs for same disease.
2.Multiple prescribers.
3.Multiple diseases.
4.Poor patient compliance .
5. Drug factors like it is not palatable or too many in frequency .
6.Multiple unknown action of drugs.
7. Most imp is patients age .
Effects of drug interaction:-
1.Quantitative i.e Increase or decrease the response intensity.
2. Qualitative:- abnormal /different type of response.
Mechanism of drug interaction :-
A.Pharmacokinetic interactions include,
1.Absorption (either complex formation ,pH change ,or alteration in motility of GIT.)
2. Distribution:- (displacement from plasma protein binding site + inhibition of metabolism /or excretion)
3. Metabolism:- ( induction of enzymes or inhibition of enzymes or hepatic blood flow)
4.Excretion:- ( alteration in urine pH, Competition for active secretion ,renal blood flow)
B. Pharmacodynamic drug interactions include,
1.Antagonism
2. Summation
3.synergism
C.Drug interaction before administration:-
Either mixing before administration.
Or, exposure to light in some cases. (Like sodium nitroprusside).
-Upasana Y.
Blood retinal Barrier
Hello :)
There are two blood retinal Barrier (BRB) :-

1. Outer blood retinal Barrier - Formed by tight junction of retinal pigmented epithelium.
2. Inner blood Retinal Barrier - Formed by Muller cells and pericytes surrounding the lining of microvasculature.
That's all for today.
-Upasana Y. :)
There are two blood retinal Barrier (BRB) :-

1. Outer blood retinal Barrier - Formed by tight junction of retinal pigmented epithelium.
2. Inner blood Retinal Barrier - Formed by Muller cells and pericytes surrounding the lining of microvasculature.
That's all for today.
-Upasana Y. :)
Thursday, August 31, 2017

Wednesday, August 30, 2017
Tuesday, August 29, 2017
Saturday, August 26, 2017
Immunology question
Hola awesomites!!
So, this is answer of our previous question. Lets have a look into it.
Q1)Which of the following features is not shared between T cells and B cells
a)Antigen specific Receptors
b)Class 1 MHC expression
c)Positive selection during development
d)All of the above
Answer is
C) Positive selection during development
Explanation:
Positive selection:
Site is thymic cortex.
-T cells having affinity for MHC molecules are selected since T cells having affinity for MHC molecules can interect with APC and one who don't have recognisation is killed
Negative selection:
Site:Thymic medulla
Selected T cells are sent to medulla,where there affinity for self antigens are tested.If the have affinity they are programmed to death.
Incase of B cells,if they recognize self antigens they do not undergo death instead there receptors are changed by the process called as "Receptor editing" .If receptor editing dose not take place,then apoptosis takes place.This is negative selection of immature B cells. B cells negative selection occurs in the bone marrow
Both T-cell and B-cell have TCRs and BCRs respectively.
Class I MHC is expressed on both T cells and B cells..
Stay awesome:)
~Ojas
Opioids analgesics classification + NEET notes
Hello awesomites so here is my " Single page notes" on opioid analgesics.
Lets begin.
Lets begin.
Let us know the difference between opiates and opioids.
Chemicals derived from opium or related to morphine chemically are called opiates.
And those having morphine like structures, irrespective of chemical action are called as opioids.
Opioid analgesics are classified as follow
1) Natural opium alkaloids
- Morphine, Codeine.
Morphine
A) Acts on Mu(Causes dependency-Euphoria) , kappa(Dysphoria - Psychomimetic) and delta receptors as agonist. Hence used as supraspinal and Spinal analgesic.
B) Treatment of poisoning: Naloxone 0.4-0.8 mg i.v. repeatedly for 2-3 minutes.
C) Can be administered through oral, rectal, i.m, i.v, intrathecal, epidural routes. Used as preanaesthetic medications
D) Useful in MI and acute pulmonary edema(Both by i.v. route)
E) Contraindicated in head injury, hypothyroidism patient, pregnancy.
A) Acts on Mu(Causes dependency-Euphoria) , kappa(Dysphoria - Psychomimetic) and delta receptors as agonist. Hence used as supraspinal and Spinal analgesic.
B) Treatment of poisoning: Naloxone 0.4-0.8 mg i.v. repeatedly for 2-3 minutes.
C) Can be administered through oral, rectal, i.m, i.v, intrathecal, epidural routes. Used as preanaesthetic medications
D) Useful in MI and acute pulmonary edema(Both by i.v. route)
E) Contraindicated in head injury, hypothyroidism patient, pregnancy.
Codeine.
A) Partial agonist at mu receptor.
B) 1/10th analgesic of morphine and less efficacious.
A) Partial agonist at mu receptor.
B) 1/10th analgesic of morphine and less efficacious.
2)Semi-syntheic opioids :
Diacetyl morphine(Heroine), Pholcodine, Ethylmorphine.
Heroine:Three time more potent than morphine.
Codeine, pholcodeine, dextromethopran and noscapine are cough suppresants.
Dextromethopran is devoid of constipating action.
Dextromethopran is devoid of constipating action.
3) Synthetic opioids:
-Pethidine(Meperidine):
A) To control shivering after anesthesia
B) Used during labour as analgesic
C) Safer in asthma.
D) Pethidine and pentazosin both are anticholinergics. Hence they causes tachycardia. Perhaps, they are contraindicated in MI but useful in biliary colic
A) To control shivering after anesthesia
B) Used during labour as analgesic
C) Safer in asthma.
D) Pethidine and pentazosin both are anticholinergics. Hence they causes tachycardia. Perhaps, they are contraindicated in MI but useful in biliary colic
-Fentanyl:
A) Causes truncal rigidity due action on mu receptor.
B) Can be given as transdermal patch and as well as buccal transmucosal
-Methadone
A) Agonist action on mu receptor + blocks NMDA reuptake of monoamines and hence useful in neuropathic and cancer pain (Not controlled by morphine)
B) Can be given by oral, rectal, i.v, s.c, routes.
C) Long plasma half-life hence less dependency and tolerance. Therefore used as maintenance therapy in opioid dependency
-Dextropropoxyphene
A) At high doses it causes seizures.
-Tramadol
A) It is a weak mu receptor agonist and decrease reuptake of NA and 5-HT hence used as analgesia. This is abolished by Ondasteron.
By ojas

Friday, August 25, 2017
MIL: Rhabdomyosarcoma of the Right Eye
Image: Rhabdomyosarcoma of the Right Eye
Submitted by: Does not wish to reveal identity
Introducing Medicowesome Image Library (MIL)
Hello everyone!
I wish to create a visual learning experience by adding images and videos along with what we write.
But since most images on Google have copyright issues, the Medicowesome authors can't use them :(
That is why, I'm asking medical students, residents and acquaintances to send me images of what they see to help create the Medicowesome Image Library (MIL).
It can be anything - a histology slide, a microbiology agar, a pathology specimen, a rash, an instrument, an x-ray - anything!
I wish to create a visual learning experience by adding images and videos along with what we write.
But since most images on Google have copyright issues, the Medicowesome authors can't use them :(
That is why, I'm asking medical students, residents and acquaintances to send me images of what they see to help create the Medicowesome Image Library (MIL).
It can be anything - a histology slide, a microbiology agar, a pathology specimen, a rash, an instrument, an x-ray - anything!
Treatment of streptococcal tonsillopharyngitis: Important points for USMLE
Hello!
Here's a quick post of treatment of "strep throat" (my slang for "Tonsillopharyngitis due to Streptococcus pyogenes, also known as group A Streptococcus.")
Here's a quick post of treatment of "strep throat" (my slang for "Tonsillopharyngitis due to Streptococcus pyogenes, also known as group A Streptococcus.")
Thursday, August 24, 2017
Question on sedative-hypnotics
Hello awesomites! Let us discuss about our previous question.
Question) Which of the following statement(s) is/are true regarding benzodiazepines?
A) It acts as GABA agonist
B) Diazepam is a short acting benzodiazepine
C) Diazepam causes lesser respiratory depression than midazolam
D) Nitrazepam is metabolized in liver
E) Diazepam has higher abuse potential than midazolam
#Pharmacology
#Medicowesome
So here is answer of our previous pharmacology question
Correct answer is C and D.
C) Diazepam causes lesser respiratory depression than midazolam
D) Nitrazepam is metabolized in liver.
Explanation:
BZDs has facilitatory action. They are not a GABA agonist.
Diazepam has rapid onset of action but prolonged action due to formation of active metabolite.
BZDs like nitrazepam, flurazepam etc are metabolised in liver by dealkylation and hydroxylation.
The dependence producing liability of BZD is low. They are Infrequently used now.
-Ojas
Classification of sedatives & hypnotics + notes for NEET
Hello awesomites!! So, here are my "Single page notes" on sedative-hypnotics. To the end of this post I have uploaded picture of my notes. So lets begin.
Classification:It is classified into 3 categories.
1)Barbiturates
Key points :
a) No antidote.Poisoning treated by gastric lavage, symptomatic treatment and forced alkaline diuresis
b) Steep curve dose.
c) Inhibits all areas of CNS. Most sensitive is reticular system
d) It inhibits all areas of CNS. Mostly reticular system which leads to inability to maintain wakefullness.
e) May cause "Hyperalgesia".
f) Duration of REM sleep and stage 3, 4 of sleep cycle decreases
g) Contraindictated in acute intermittent porphyria
i) Hangover is common
Barbiturates are further classified into three types.
a) No antidote.Poisoning treated by gastric lavage, symptomatic treatment and forced alkaline diuresis
b) Steep curve dose.
c) Inhibits all areas of CNS. Most sensitive is reticular system
d) It inhibits all areas of CNS. Mostly reticular system which leads to inability to maintain wakefullness.
e) May cause "Hyperalgesia".
f) Duration of REM sleep and stage 3, 4 of sleep cycle decreases
g) Contraindictated in acute intermittent porphyria
i) Hangover is common
Barbiturates are further classified into three types.
A) Long acting
Phenobarbitone.
B) Short acting.
Butobarbitone
Pentobarbitone.
Butobarbitone
Pentobarbitone.
C) Ultra short acting
Thiopentone.
Methohexitone.
Thiopentone.
Methohexitone.
2)Benzodiazepines
Key points:
a) Antidote:Flumazenil is competitive antagonist. It takes 30-60 minutes for its action.
b) Flat dose curve.
c) Duration of REM sleep decreases but frequency increases.
d) Hangover less common
They are further classified into three categories
a) Antidote:Flumazenil is competitive antagonist. It takes 30-60 minutes for its action.
b) Flat dose curve.
c) Duration of REM sleep decreases but frequency increases.
d) Hangover less common
They are further classified into three categories
A) Hypnotics
-Diazepam:Causes analgesia(Barbiturates causes hyperalgesia as mentioned earlier.) and it also causes muscle relaxation
-Flurazepam :Paradoxical simulation and increase nightmare
-Nitrazepam:Increase REM sleep (Rest decreases)
-Temazepam
-Flunitrazepam : Tasteless BZD called as "
" Date rape drug"
-Midazolam:Causes blackouts and ataxia.
-Alprazolam
-Triazolam:Responsible for paranoia and other psychiatric disturbances.
-Flurazepam :Paradoxical simulation and increase nightmare
-Nitrazepam:Increase REM sleep (Rest decreases)
-Temazepam
-Flunitrazepam : Tasteless BZD called as "
" Date rape drug"
-Midazolam:Causes blackouts and ataxia.
-Alprazolam
-Triazolam:Responsible for paranoia and other psychiatric disturbances.
B)Anti-anxiety
Remember OLA-CD
-Oxazepam
-Lorazepam:Absorption from intramuscular site is regular for other drugs its irregular.
-Alprazolam
-Chlordiazepoxide.
-Diazepam.
-Lorazepam:Absorption from intramuscular site is regular for other drugs its irregular.
-Alprazolam
-Chlordiazepoxide.
-Diazepam.
C) Anti-convulsants :
-Diazepam
-Lorazepam
-Clonazepam
-Clobazam
-Lorazepam
-Clonazepam
-Clobazam
Remember: EasT LOT
E=Estazolam
T=Temazepam
L=Lorazepam
O=Oxazepam
T=Triazolam
E=Estazolam
T=Temazepam
L=Lorazepam
O=Oxazepam
T=Triazolam
These drugs directly conjugated without metabolism to active products. These are short acting and can be used in liver failure
3)Newer non-benzodiazepine hypnotics:
-Zopiclone:
a) Increases stage 3 and stage 4 duration
b) Indicated for patients BZDs for induction of sleep
c) Less rebound insomnia and hangover.
b) Active metabolite is eszopiclone.
c) Less rebound insomnia and hangover.
b) Active metabolite is eszopiclone.
-Zolpidem
a) Lacks anti-anxiety, muscle relaxants, and anti-convulsants actions.
b) Use in short term treatment of insomnia.
c) No rebound insomnia and hangover.
a) Lacks anti-anxiety, muscle relaxants, and anti-convulsants actions.
b) Use in short term treatment of insomnia.
c) No rebound insomnia and hangover.
-Zaleplon
a) Decreases sleep latency without affecting sleep time.
a) Decreases sleep latency without affecting sleep time.
-Suvorexant:
a) Its is Orexin antagonist. Orexin is wake-fullness receptor.
a) Its is Orexin antagonist. Orexin is wake-fullness receptor.
Ojas

Wednesday, August 23, 2017


Tuesday, August 22, 2017
Image Based MCQ on Instruments
Hello awesomites!
Yesterday we posted an Image based MCQ on Instruments and here is the answer to the question.
#Image_based
#Instruments
Q. What is the inner diameter of the device shown in the picture if it is to be used in adults?

A. 2-3 mm
B. 8-9 mm
C. 12-15 mm
D. 21-23 mm
The correct answer is B. 8-9 mm. The image given shows an Endotracheal tube that is available in different sizes for different age groups.
Internal diameter 3mm - 6mm is used for Paediatric cases.
Typically, an 8.0 or 8.5 mm for adult men and 7.5 to 8.0 mm for adult women is an ideal choice.
B. 8-9 mm
C. 12-15 mm
D. 21-23 mm
The correct answer is B. 8-9 mm. The image given shows an Endotracheal tube that is available in different sizes for different age groups.
Internal diameter 3mm - 6mm is used for Paediatric cases.
Typically, an 8.0 or 8.5 mm for adult men and 7.5 to 8.0 mm for adult women is an ideal choice.
Thanks for your active participation in the question.
MD Mobarak Hussain (Maahii)
Monday, August 21, 2017
Cushing Vs Curling Ulcer
Hello!
Its time to differentiate between two confusing ulcers - Cushing and Curling.
What is Cushing Reflex?
It is a triad of Bradycardia, Hypertension and altered respiration following Head injury.
What is Cushing Ulcer?
Stress Ulcer following Head injury.
Most common site - Acid producing area of Stomach.
What is Curling Ulcer?
Stress Ulcer following Burn.
Thomas Blizzard Curling.
Reduced plasma volume leads to ischemia and cell necrosis of the mucosa.
Most common site - 1st part of Duodenum.
cURling = bURn
This may help you to remember the difference between these two.
Thanks
MD Mobarak Hussain (Maahii)
Latanoprost and Pilocarpine never go together
Latanoprost increases the uveoscleral outflow of the aqueous humor. Pilocarpine has a constrictive effect on the ciliary body as a whole. Hence, when the two are used together, their effects end up getting nullified with the physician bungling to achieve the target IOP.
That's all!
-Sushrut Dongargaonkar
Introducing Medicollabowesome

Hello everyone!
We, the Medicowesome authors, decided to do something new this month and bring to you - Medicollabowesome.
The idea originated from wanting to see how different people present information uniquely on the same topic.
The Medicowesome authors decided that most of us will (try) to write on one particular topic every month.
Hopefully, we will learn so much together :D
The topic for the month of August: HIV & AIDS.
We've already begun writing (:
I invite readers to participate in Medicollabowesome too by emailing your article to us!
Email the title, post and author name to medicowesome@gmail.com with "Medicollabowesome" in the subject line.
This is so exciting!
-IkaN
Sunday, August 20, 2017
Saturday, August 19, 2017
Friday, August 18, 2017
Drug of choice : Dermatology
Hello everyone!
Here's a collection of Drugs of choice (DOC) for some Dermatology conditions. These are some of the most commonly asked questions in Post Graduation entrance exams.
1. DOC for severe erythrodermic psoriasis?
Cyclosporin
2. DOC for erythrodermic psoriasis?Methotrexate
3. DOC for pustular psoriasis?
Acitretin
4. 2nd choice for pustular psoriasis?Methotrexate
5. DOC for arthritis mutilans?
Etanercept
6. DOC for impetigo herpetiformis?
Systemic steroids
7. DOC for psoriatic arthritis?
Methotrexate
8. DOC for psoriatic erythroderma in pregnancy?
Systemic steroid
-Md Mobarak Hussain (Maahii)
Thursday, August 17, 2017
Clubbing
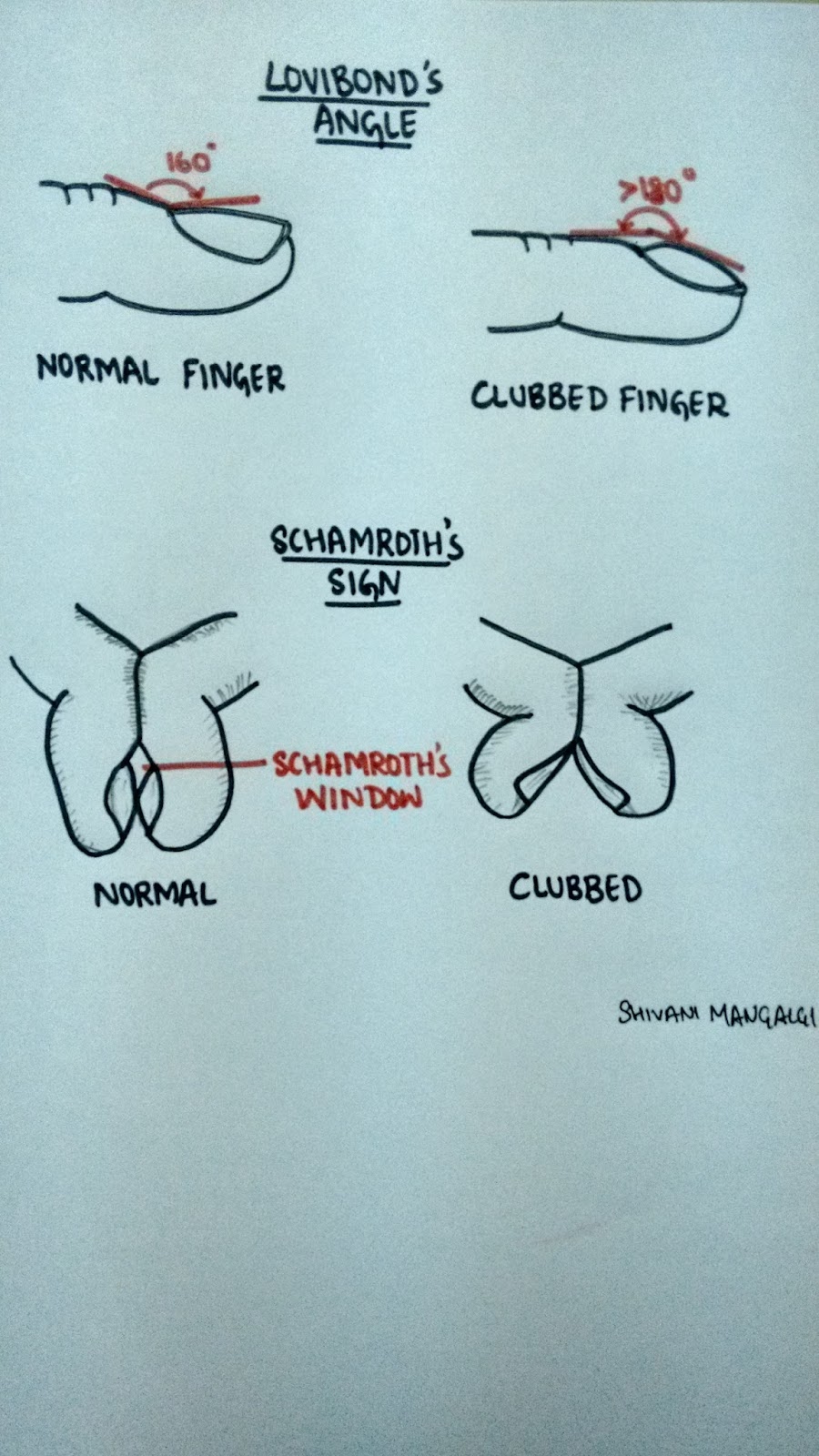
CLUBBING:
Bulbous enlargement of the distal portion of the digits due to increased subungual soft tissue.
It is also known as the "Hippocratic fingers", as it is believed that perhaps Hippocrates was the first to document clubbing as a sign of disease.
Grades of clubbing-
Grade I- presence of fluctuation test °
Grade II- obliteration of Lovibond angle*
Grade III- parrot beak or drumstick appearance
Grade IV- hypertrophic osteoarthropathy (HOA)
*Refer the diagram
°Refer the video clipping
Theories of clubbing-
1. Neurogenic theory- vagal stimulation via neural reflexes can lead to proliferation of connective tissue at the distal extremities resulting in clubbing.
2.Humoral theory- Normally lungs throws out all the soluble substances by inactivation. But in case of lung problems, these systems reach the systemic circulation in active state and stimulate the changes seen in HOA (growth hormone, PTH, bradikynin, prostaglandin, ferritin)
3.Hypoxic theory- Hypoxia is suggested to be a stimulus for HOA. It leads to opening of deep arteriovenous shunts and fistulae which increase blood flow to the extremities and leads to hypertrophy.
4.Platelets derived growth factor- Normally megakaryocytes and large platelets get destroyed in the lungs. But in lung pathology they escape the lung and reach the distal extremities. Here they interact with the endothelial cells and release platelet derives growth factor (PDGF) post activation. PDGF and other mediators then activate the fibroblasts and transforming growth factor beta which lead to collagen production and connective tissue laying down ultimately giving rise to clubbing and HOA.
This is the latest accepted theory.
Causes of clubbing-
'CLUBBING'
C - cyanotic heart diseases, chron's disease
L - lung causes (lung abscess, emphysema, interstitial lung disease, bronchogenic carcinoma, tuberculosis)
U - ulcerative colitis
B - biliary cirrhosis
B - benign mesothelioma
I - infective endocarditis, idiopathic, inherited
N - neurogenic tumors
G - graves disease
Shivani Mangalgi
Medicowesome 2017

Bulbous enlargement of the distal portion of the digits due to increased subungual soft tissue.
It is also known as the "Hippocratic fingers", as it is believed that perhaps Hippocrates was the first to document clubbing as a sign of disease.
Grades of clubbing-
Grade I- presence of fluctuation test °
Grade II- obliteration of Lovibond angle*
Grade III- parrot beak or drumstick appearance
Grade IV- hypertrophic osteoarthropathy (HOA)
*Refer the diagram
°Refer the video clipping
Theories of clubbing-
1. Neurogenic theory- vagal stimulation via neural reflexes can lead to proliferation of connective tissue at the distal extremities resulting in clubbing.
2.Humoral theory- Normally lungs throws out all the soluble substances by inactivation. But in case of lung problems, these systems reach the systemic circulation in active state and stimulate the changes seen in HOA (growth hormone, PTH, bradikynin, prostaglandin, ferritin)
3.Hypoxic theory- Hypoxia is suggested to be a stimulus for HOA. It leads to opening of deep arteriovenous shunts and fistulae which increase blood flow to the extremities and leads to hypertrophy.
4.Platelets derived growth factor- Normally megakaryocytes and large platelets get destroyed in the lungs. But in lung pathology they escape the lung and reach the distal extremities. Here they interact with the endothelial cells and release platelet derives growth factor (PDGF) post activation. PDGF and other mediators then activate the fibroblasts and transforming growth factor beta which lead to collagen production and connective tissue laying down ultimately giving rise to clubbing and HOA.
This is the latest accepted theory.
Causes of clubbing-
'CLUBBING'
C - cyanotic heart diseases, chron's disease
L - lung causes (lung abscess, emphysema, interstitial lung disease, bronchogenic carcinoma, tuberculosis)
U - ulcerative colitis
B - biliary cirrhosis
B - benign mesothelioma
I - infective endocarditis, idiopathic, inherited
N - neurogenic tumors
G - graves disease
Shivani Mangalgi
Medicowesome 2017
Courtesy YouTube
Hypergraphia - An intriguing brain anomaly
HYPERGRAPHIA
It is a condition in which an individual feels the driving compulsion to write; the overwhelming urge to write.
Hypergraphia has also been called 'midnight disease'.
Well based on how we perceive it, the "disease" could either be all about writing or writer's block.
Neurologically-
This unstoppable drive to write can be triggered by temporal lobe epilepsy(hippocampus and Wernicke's area in specific), intolerant mood disorders or dopamine.
What is very fascinating about this condition is that there are NO other vicious symptoms (other than a little irritability-which is quiet expected) and the fact that the patient can go on writing on anything from toilet papers to wall to even roads.
And what is more fascinating to know is that many famous authors and poets like Sylvia Plath, Stephen King and Leo Tolstoy (that's how the world got "War and Peace") suffered from hypergraphia.
Ingenious result from a brain defect.
Now a question might arise..if the quality of writing in these patients is any good?
To answer this, it is important to know that patient with hypergraphia exhibit wide variety of writing style and content. To elucidate this statement, let's go through few accounts:
1. Alice Flaherty (Harvard Medical school neurologist) gets episodes of hypergraphia following any grief incidences that have grave affect on her brain.
She has started her 4th book and is doing research to help explain how the muse comes and goes.
2. Mendez- He felt the unreasonable compulsion to write poetry even though the patient had no previous history of being a poet.
3. Patient who wrote everything backwards!
4. Patients writing same word over and over again but with differing calligraphy.
5. Patients' writing consists of sheer scribbling and frantic random thoughts.
Therefore on a lighter note, if you have the wrong brain defect but fall under the right category...then voilà...YOU shall be famous!
Shivani Mangalgi
Medicowesome 2017
It is a condition in which an individual feels the driving compulsion to write; the overwhelming urge to write.
Hypergraphia has also been called 'midnight disease'.
Well based on how we perceive it, the "disease" could either be all about writing or writer's block.
Neurologically-
This unstoppable drive to write can be triggered by temporal lobe epilepsy(hippocampus and Wernicke's area in specific), intolerant mood disorders or dopamine.
What is very fascinating about this condition is that there are NO other vicious symptoms (other than a little irritability-which is quiet expected) and the fact that the patient can go on writing on anything from toilet papers to wall to even roads.
And what is more fascinating to know is that many famous authors and poets like Sylvia Plath, Stephen King and Leo Tolstoy (that's how the world got "War and Peace") suffered from hypergraphia.
Ingenious result from a brain defect.
Now a question might arise..if the quality of writing in these patients is any good?
To answer this, it is important to know that patient with hypergraphia exhibit wide variety of writing style and content. To elucidate this statement, let's go through few accounts:
1. Alice Flaherty (Harvard Medical school neurologist) gets episodes of hypergraphia following any grief incidences that have grave affect on her brain.
She has started her 4th book and is doing research to help explain how the muse comes and goes.
2. Mendez- He felt the unreasonable compulsion to write poetry even though the patient had no previous history of being a poet.
3. Patient who wrote everything backwards!
4. Patients writing same word over and over again but with differing calligraphy.
5. Patients' writing consists of sheer scribbling and frantic random thoughts.
Therefore on a lighter note, if you have the wrong brain defect but fall under the right category...then voilà...YOU shall be famous!
Shivani Mangalgi
Medicowesome 2017
Subscribe to:
Comments (Atom)