
Thursday, August 31, 2017

Wednesday, August 30, 2017
Tuesday, August 29, 2017
Saturday, August 26, 2017
Immunology question
Hola awesomites!!
So, this is answer of our previous question. Lets have a look into it.
Q1)Which of the following features is not shared between T cells and B cells
a)Antigen specific Receptors
b)Class 1 MHC expression
c)Positive selection during development
d)All of the above
Answer is
C) Positive selection during development
Explanation:
Positive selection:
Site is thymic cortex.
-T cells having affinity for MHC molecules are selected since T cells having affinity for MHC molecules can interect with APC and one who don't have recognisation is killed
Negative selection:
Site:Thymic medulla
Selected T cells are sent to medulla,where there affinity for self antigens are tested.If the have affinity they are programmed to death.
Incase of B cells,if they recognize self antigens they do not undergo death instead there receptors are changed by the process called as "Receptor editing" .If receptor editing dose not take place,then apoptosis takes place.This is negative selection of immature B cells. B cells negative selection occurs in the bone marrow
Both T-cell and B-cell have TCRs and BCRs respectively.
Class I MHC is expressed on both T cells and B cells..
Stay awesome:)
~Ojas
Opioids analgesics classification + NEET notes
Lets begin.
Chemicals derived from opium or related to morphine chemically are called opiates.
1) Natural opium alkaloids
- Morphine, Codeine.
A) Acts on Mu(Causes dependency-Euphoria) , kappa(Dysphoria - Psychomimetic) and delta receptors as agonist. Hence used as supraspinal and Spinal analgesic.
B) Treatment of poisoning: Naloxone 0.4-0.8 mg i.v. repeatedly for 2-3 minutes.
C) Can be administered through oral, rectal, i.m, i.v, intrathecal, epidural routes. Used as preanaesthetic medications
D) Useful in MI and acute pulmonary edema(Both by i.v. route)
E) Contraindicated in head injury, hypothyroidism patient, pregnancy.
A) Partial agonist at mu receptor.
B) 1/10th analgesic of morphine and less efficacious.
Diacetyl morphine(Heroine), Pholcodine, Ethylmorphine.
Dextromethopran is devoid of constipating action.
A) To control shivering after anesthesia
B) Used during labour as analgesic
C) Safer in asthma.
D) Pethidine and pentazosin both are anticholinergics. Hence they causes tachycardia. Perhaps, they are contraindicated in MI but useful in biliary colic
A) Causes truncal rigidity due action on mu receptor.
B) Can be given as transdermal patch and as well as buccal transmucosal
A) Agonist action on mu receptor + blocks NMDA reuptake of monoamines and hence useful in neuropathic and cancer pain (Not controlled by morphine)
B) Can be given by oral, rectal, i.v, s.c, routes.
C) Long plasma half-life hence less dependency and tolerance. Therefore used as maintenance therapy in opioid dependency
A) It is a weak mu receptor agonist and decrease reuptake of NA and 5-HT hence used as analgesia. This is abolished by Ondasteron.

Friday, August 25, 2017
MIL: Rhabdomyosarcoma of the Right Eye
Introducing Medicowesome Image Library (MIL)
I wish to create a visual learning experience by adding images and videos along with what we write.
But since most images on Google have copyright issues, the Medicowesome authors can't use them :(
That is why, I'm asking medical students, residents and acquaintances to send me images of what they see to help create the Medicowesome Image Library (MIL).
It can be anything - a histology slide, a microbiology agar, a pathology specimen, a rash, an instrument, an x-ray - anything!
Treatment of streptococcal tonsillopharyngitis: Important points for USMLE
Here's a quick post of treatment of "strep throat" (my slang for "Tonsillopharyngitis due to Streptococcus pyogenes, also known as group A Streptococcus.")
Thursday, August 24, 2017
Question on sedative-hypnotics
Hello awesomites! Let us discuss about our previous question.
Question) Which of the following statement(s) is/are true regarding benzodiazepines?
A) It acts as GABA agonist
B) Diazepam is a short acting benzodiazepine
C) Diazepam causes lesser respiratory depression than midazolam
D) Nitrazepam is metabolized in liver
E) Diazepam has higher abuse potential than midazolam
#Pharmacology
#Medicowesome
So here is answer of our previous pharmacology question
Correct answer is C and D.
C) Diazepam causes lesser respiratory depression than midazolam
D) Nitrazepam is metabolized in liver.
Explanation:
BZDs has facilitatory action. They are not a GABA agonist.
Diazepam has rapid onset of action but prolonged action due to formation of active metabolite.
BZDs like nitrazepam, flurazepam etc are metabolised in liver by dealkylation and hydroxylation.
The dependence producing liability of BZD is low. They are Infrequently used now.
-Ojas
Classification of sedatives & hypnotics + notes for NEET
a) No antidote.Poisoning treated by gastric lavage, symptomatic treatment and forced alkaline diuresis
b) Steep curve dose.
c) Inhibits all areas of CNS. Most sensitive is reticular system
d) It inhibits all areas of CNS. Mostly reticular system which leads to inability to maintain wakefullness.
e) May cause "Hyperalgesia".
f) Duration of REM sleep and stage 3, 4 of sleep cycle decreases
g) Contraindictated in acute intermittent porphyria
i) Hangover is common
Barbiturates are further classified into three types.
A) Long acting
Phenobarbitone.
Butobarbitone
Pentobarbitone.
Thiopentone.
Methohexitone.
a) Antidote:Flumazenil is competitive antagonist. It takes 30-60 minutes for its action.
b) Flat dose curve.
c) Duration of REM sleep decreases but frequency increases.
d) Hangover less common
They are further classified into three categories
-Flurazepam :Paradoxical simulation and increase nightmare
-Nitrazepam:Increase REM sleep (Rest decreases)
-Temazepam
-Flunitrazepam : Tasteless BZD called as "
" Date rape drug"
-Midazolam:Causes blackouts and ataxia.
-Alprazolam
-Triazolam:Responsible for paranoia and other psychiatric disturbances.
-Lorazepam:Absorption from intramuscular site is regular for other drugs its irregular.
-Alprazolam
-Chlordiazepoxide.
-Diazepam.
-Lorazepam
-Clonazepam
-Clobazam
E=Estazolam
T=Temazepam
L=Lorazepam
O=Oxazepam
T=Triazolam
c) Less rebound insomnia and hangover.
b) Active metabolite is eszopiclone.
a) Lacks anti-anxiety, muscle relaxants, and anti-convulsants actions.
b) Use in short term treatment of insomnia.
c) No rebound insomnia and hangover.
a) Decreases sleep latency without affecting sleep time.
a) Its is Orexin antagonist. Orexin is wake-fullness receptor.

Wednesday, August 23, 2017


Tuesday, August 22, 2017
Image Based MCQ on Instruments
Hello awesomites!
Yesterday we posted an Image based MCQ on Instruments and here is the answer to the question.
#Image_based
#Instruments
Q. What is the inner diameter of the device shown in the picture if it is to be used in adults?

B. 8-9 mm
C. 12-15 mm
D. 21-23 mm
The correct answer is B. 8-9 mm. The image given shows an Endotracheal tube that is available in different sizes for different age groups.
Internal diameter 3mm - 6mm is used for Paediatric cases.
Typically, an 8.0 or 8.5 mm for adult men and 7.5 to 8.0 mm for adult women is an ideal choice.
Monday, August 21, 2017
Cushing Vs Curling Ulcer
Hello!
Its time to differentiate between two confusing ulcers - Cushing and Curling.
What is Cushing Reflex?
It is a triad of Bradycardia, Hypertension and altered respiration following Head injury.
What is Cushing Ulcer?
Stress Ulcer following Head injury.
Most common site - Acid producing area of Stomach.
What is Curling Ulcer?
Stress Ulcer following Burn.
Thomas Blizzard Curling.
Reduced plasma volume leads to ischemia and cell necrosis of the mucosa.
Most common site - 1st part of Duodenum.
cURling = bURn
This may help you to remember the difference between these two.
Thanks
MD Mobarak Hussain (Maahii)
Latanoprost and Pilocarpine never go together
Latanoprost increases the uveoscleral outflow of the aqueous humor. Pilocarpine has a constrictive effect on the ciliary body as a whole. Hence, when the two are used together, their effects end up getting nullified with the physician bungling to achieve the target IOP.
That's all!
-Sushrut Dongargaonkar
Introducing Medicollabowesome

Hello everyone!
We, the Medicowesome authors, decided to do something new this month and bring to you - Medicollabowesome.
Sunday, August 20, 2017
Saturday, August 19, 2017
Friday, August 18, 2017
Drug of choice : Dermatology
Hello everyone!
Here's a collection of Drugs of choice (DOC) for some Dermatology conditions. These are some of the most commonly asked questions in Post Graduation entrance exams.
1. DOC for severe erythrodermic psoriasis?
Cyclosporin
2. DOC for erythrodermic psoriasis?Methotrexate
3. DOC for pustular psoriasis?
Acitretin
4. 2nd choice for pustular psoriasis?Methotrexate
5. DOC for arthritis mutilans?
Etanercept
6. DOC for impetigo herpetiformis?
Systemic steroids
7. DOC for psoriatic arthritis?
Methotrexate
8. DOC for psoriatic erythroderma in pregnancy?
Systemic steroid
-Md Mobarak Hussain (Maahii)
Thursday, August 17, 2017
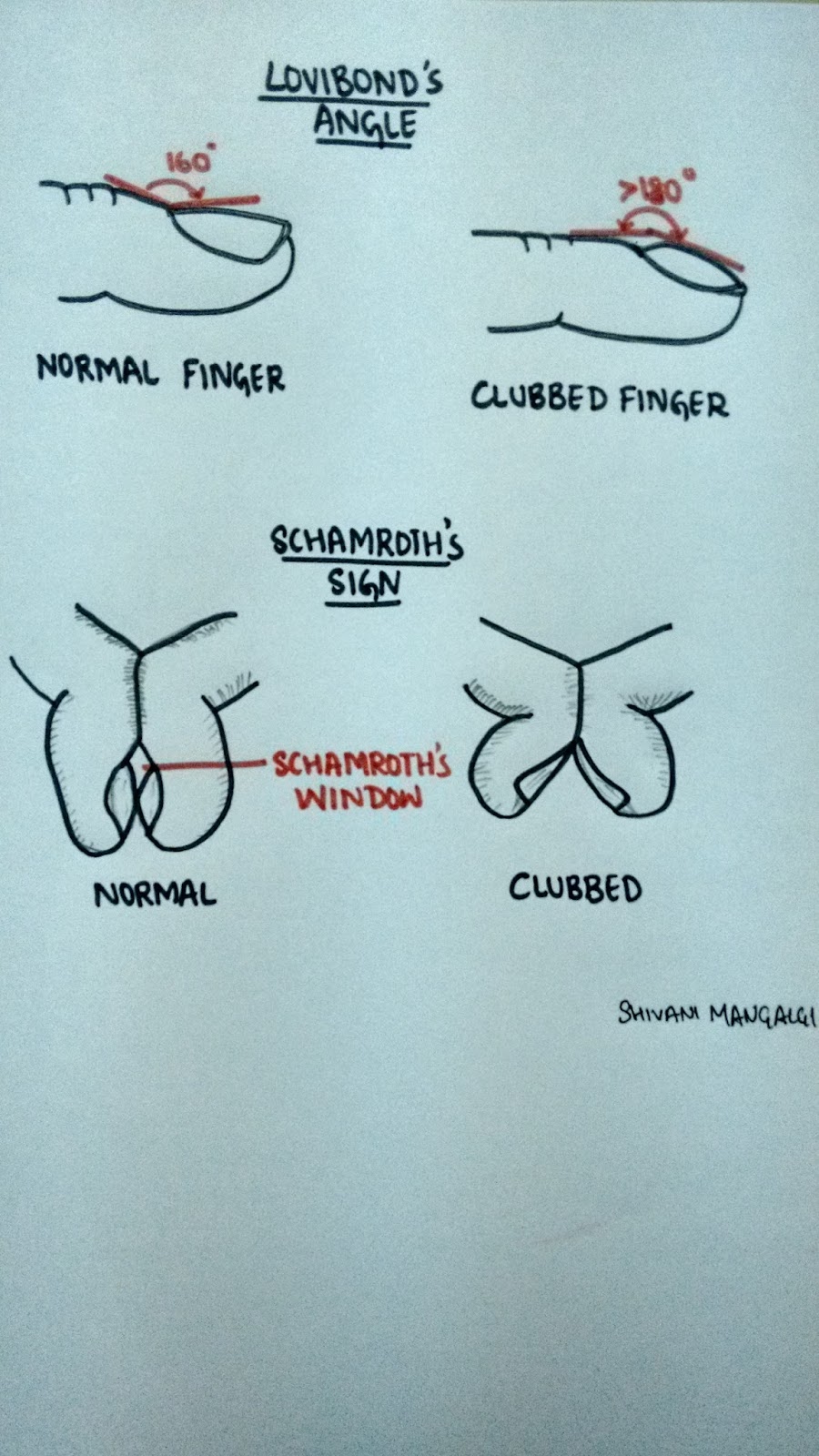
Clubbing
Bulbous enlargement of the distal portion of the digits due to increased subungual soft tissue.
It is also known as the "Hippocratic fingers", as it is believed that perhaps Hippocrates was the first to document clubbing as a sign of disease.
Grades of clubbing-
Grade I- presence of fluctuation test °
Grade II- obliteration of Lovibond angle*
Grade III- parrot beak or drumstick appearance
Grade IV- hypertrophic osteoarthropathy (HOA)
*Refer the diagram
°Refer the video clipping
Theories of clubbing-
1. Neurogenic theory- vagal stimulation via neural reflexes can lead to proliferation of connective tissue at the distal extremities resulting in clubbing.
2.Humoral theory- Normally lungs throws out all the soluble substances by inactivation. But in case of lung problems, these systems reach the systemic circulation in active state and stimulate the changes seen in HOA (growth hormone, PTH, bradikynin, prostaglandin, ferritin)
3.Hypoxic theory- Hypoxia is suggested to be a stimulus for HOA. It leads to opening of deep arteriovenous shunts and fistulae which increase blood flow to the extremities and leads to hypertrophy.
4.Platelets derived growth factor- Normally megakaryocytes and large platelets get destroyed in the lungs. But in lung pathology they escape the lung and reach the distal extremities. Here they interact with the endothelial cells and release platelet derives growth factor (PDGF) post activation. PDGF and other mediators then activate the fibroblasts and transforming growth factor beta which lead to collagen production and connective tissue laying down ultimately giving rise to clubbing and HOA.
This is the latest accepted theory.
Causes of clubbing-
'CLUBBING'
C - cyanotic heart diseases, chron's disease
L - lung causes (lung abscess, emphysema, interstitial lung disease, bronchogenic carcinoma, tuberculosis)
U - ulcerative colitis
B - biliary cirrhosis
B - benign mesothelioma
I - infective endocarditis, idiopathic, inherited
N - neurogenic tumors
G - graves disease
Shivani Mangalgi
Medicowesome 2017
Hypergraphia - An intriguing brain anomaly
It is a condition in which an individual feels the driving compulsion to write; the overwhelming urge to write.
Hypergraphia has also been called 'midnight disease'.
Well based on how we perceive it, the "disease" could either be all about writing or writer's block.
Neurologically-
This unstoppable drive to write can be triggered by temporal lobe epilepsy(hippocampus and Wernicke's area in specific), intolerant mood disorders or dopamine.
What is very fascinating about this condition is that there are NO other vicious symptoms (other than a little irritability-which is quiet expected) and the fact that the patient can go on writing on anything from toilet papers to wall to even roads.
And what is more fascinating to know is that many famous authors and poets like Sylvia Plath, Stephen King and Leo Tolstoy (that's how the world got "War and Peace") suffered from hypergraphia.
Ingenious result from a brain defect.
Now a question might arise..if the quality of writing in these patients is any good?
To answer this, it is important to know that patient with hypergraphia exhibit wide variety of writing style and content. To elucidate this statement, let's go through few accounts:
1. Alice Flaherty (Harvard Medical school neurologist) gets episodes of hypergraphia following any grief incidences that have grave affect on her brain.
She has started her 4th book and is doing research to help explain how the muse comes and goes.
2. Mendez- He felt the unreasonable compulsion to write poetry even though the patient had no previous history of being a poet.
3. Patient who wrote everything backwards!
4. Patients writing same word over and over again but with differing calligraphy.
5. Patients' writing consists of sheer scribbling and frantic random thoughts.
Therefore on a lighter note, if you have the wrong brain defect but fall under the right category...then voilà...YOU shall be famous!
Shivani Mangalgi
Medicowesome 2017
Leucocoria
Also known as the white pupillary reflex, is an abnormal white reflection from the retina of the eye.
Pathologically it's the absence of the red reflex.
Clinically the pupils appear white rather than the usual black color.
Mnemonic for causes of leukocoria-
'CREAM PIGMENT'
C - Coats disease/ Coloboma/ Cataract
R - Retinoblastoma/ Retinal dysplasia/ ROP/ Retinal fold
E - Endophthalmitis
A - Astrocytic hamartoma/ Anisometropia
M - Myelinated retinal nerve fiber layer
P - Persistent fetal vasculature/ PHPV
I - Incontinentia pigmenti/ Inflammation (uveitis)
G - Granuloma
M - Melanoma/ Medulloepithelioma
E - Familial exudative vitreoretinopathy (FEVR)
N - Norrie
T - Trauma/ Toxocariasis
Go ahead and add more causes to make your own list!
Shivani Mangalgi
Medicowesome 2017
Post operative ileus ( mechanical obstruction vs paralytic )
- No return of bowel movements ( on auscultation ) after 72 hours
- Absence of flatus or stool on day 6 after surgery
- Feeling of discomfort, nausea or vomiting on oral intake, thus requiring i.v. support, NG tube placement by PO day 5.
- Partial return of bowel movements after PO day 5.
( Refer to UpToDate)
Hope this helps :)
Wednesday, August 16, 2017
Causative microbes in acute osteomyelitis
Hello Awesomites!
Let's discuss some facts about Common microbes involved in Acute Osteomyelitis.
Staphylococcus aureus is the most common infecting organism found in older children and adults with osteomyelitis.
Gram negative bacteria - vertebral body infections in adults.
Pseudomonas - intravenous drug abusers.
Fungal osteomyelitis - chronically ill patients receiving long-term intravenous therapy or parenteral nutrition.
Salmonella osteomyelitis - Sickle cell hemoglobinopathies - tends to be diaphyseal.
Infants -S. aureus (most common),group B streptococcus & gram-negative coliforms .
Group B streptococcus - otherwise healthy infants 2 to 4 weeks of age.
Animal Bite - Pasteurella
Human Bite - Eikinella
That's all!
Thank you.
MD Mobarak Hussain (Maahii)
Tuesday, August 15, 2017
Paramedian pontine reticular formation and MLF

-Upasana Y. :)

Third nerve palsy
Before starting with the III nerve, Let us understand the term.
According to TABER'S medical dictionary, We need to understand 3 main type of palsy here.
1.NUCLEAR palsy :- Paralysis caused by lesion of the nuclei in CNS.
2.OCULAR palsy :- Paralysis of extraocular nd intraocular muscles.
3.MUSCULAR palsy :- Loss of the capacity of muscle to contract. It may be due to structural or functional disorders
-in the muscle at the myoneural junction,
-in efferent nerve fibres,
-in the cell bodies of nuclei of origin of the brain or of the gray matter of the spinal cord,
-in conducting pathways of the brain or spinal cord,
-in motor centres of the brain.
Third cranial nerve supplies
1. EXTRAOCULAR MUSCLES
-Superior rectus
-Inferior oblique
-Medial rectus
-Inferior rectus
2.INTRAOCULAR MUSCLES
-Levator palpebral superioris
-Ciliary body
-Iris sphincter msucle
THE LOCALIZATION OF THIRD NERVE LESION
-Supranuclear
-Nuclear
-Fascicular
-Basilar
-Intra-Cavernous sinus
-Superior orbital fissure
-Intra Orbital part
CLINICAL FEATURES OF THIRD NERVE PALSY:-
1. Ptosis - paralysis of LPS muscle.
2. Deviation – out, down and intorted (unopposed action of LR and SO).
3. Ocular movements:
• Adduction – MR
• Elevation – SR and IO
• Depression – IR
• Extorsion – IR and IO
4. Pupil is fixed and dilated – paralysis of sphincter pupillae muscle.
5. Accommodation is completely lost – paralysis of ciliary muscle.
6. Crossed diplopia – paralytic divergent squint.
7. Head posture – If the pupillary area is uncovered, head takes a posture consistent with the directions of actions of the paralysed muscles, i.e., head is turned on the opposite side, tilted towards the same side and chin is slightly raised. (Pathways between vestibular nuclei and oculomotor nuclei. These are Intranuclear pathway.)
FEATURES AND CAUSES OF THIRD NERVE LESIONS AT VARIOUS LEVELS
1. Supranuclear lesions
• Lesions of the cerebral cortex and supranuclear pathway produce conjugate paresis which affect both eyes equally.
• In supranuclear lesions although position and movements of the eyes are abnormal, they maintain their relative co-ordination and produce no diplopia.
2. Nuclear lesions
• Lesions involving purely the third nerve nucleus are relatively uncommon.
• Common causes include ; vascular diseases, demyelination, primary tumors and metastasis
• Lesions involving entire nucleus cause
-an ipsilateral third nerve palsy with ipsilateral sparing and
-contralateral weakness of elevation.
• Lesions involving paired medial rectus subnuclei (ventromedial nucleus) cause a wall-eyed bilateral internuclear ophthalmoplegia ( WEBINO ) characterised by defective convergence and adduction.
-PULSATILE EXOPHTHALMOS can also be seen.
• Causes :
I want to thank my teacher for such a beautiful explanation.
I hope it helped.
Do read about the following . (though I will write on this topic also)
1.Injury of Paramedian pontine reticular formation
2. Ptosis in Horner's syndrome and oculomotor nerve palsy.
Drugs that can cause TOXIC MYOPATHIES
1. TYPE- Inflammatory
-Cimetidine
-D- Penicillamine
-Procainamide
-L-tryptophan
-Levodopa
2.TYPE- Non-Inflammatory necrotizing or vacuolar
-Alcohol
-Cholestrol lowering agents
-Chloroquine
-Colchicine
-Cyclosporine and tacrolimus
-Emetine
-Isoretinoic acid
-Vincristine
-Labetalol
3.TYPE -Rhabdomyolysis and myoglobinuria
-Alcohol
-Amphetamine
-Cocaine
-Heroin
-Phencyclidine
-Meperidine
4.TYPE -myosin loss
-Non depolarizing neuromuscular blocking agent
-steroid
That's all.
-Upasana Y. :)
Monday, August 14, 2017
ABC vs CAB for CPR
If someone ask the medical personnel, What is ABC ?
Unfailingly, the answer will be A-airway, B-breathing ,C-Circulation.
But now this has been changed to C-A-B.(I didn't know this)
C-Compression /circulation
A-airway
B-breathing
(SOURCE :- I took the following content from https://medictests.com/abc-vs-cab-correct/ )
In 2010 the AHA made a radical change to how we approach CPR. Up until then we all lived by the trusty "ABC" (Airway, Breathing, Circulation) method of resuscitation. Not surprisingly, though, the AHA's ongoing research began to show that compressions are the most important part of CPR and any delay or interruption resulted in worse outcomes. It was also discovered that during CPR, the patient's blood stays oxygenated for 4-6 minutes after their last breath. In response to this research, and in an attempt to simplify CPR for untrained laypeople, the AHA decided to switch our initial approach from ABC to CAB. While this change is medically sound, it has cause a lot of confusion for healthcare professionals who regularly use ABC for other scenarios. So, ABC vs CAB, which is correct?
With indisputable evidence that compressions are the most important part of CPR, it is no wonder that AHA has been dee-mphasizing airway and breathing. In fact, in ACLS, the AHA has gone as far as to suggest that endotracheal intubation may not be as important as we once thought. While it remains the ultimate airway, the AHA suggests BVM or supraglottic airway ventilations because they reduce the interruption of compressions.
In accordance with this paradigm shift, the AHA has changed ABC to CAB in the event of cardiac arrest. Unfortunately, though, some healthcare providers have incorrectly interpreted this change in cardiac arrest to be a change that applies to every other medical call. Some are under the impression that the AHA is the governing body over prehospital and emergency care, which is simply not the case. CAB is no doubt a revolution in cardiac arrest care but it is not meant to change the way we approach our "normal" patients.
Here is a short list of examples of when ABC vs CAB should be used
ABC
Overdose
Trauma
Altered mental status
Diabetic emergencies
Respiratory failure
Airway obstruction
Respiratory Distress
CAB
Cardiac Arrest
Conclusion:-
It does not have to be one or the other! While ABC has been phased out by the AHA, it still is the de facto initial assessment used in every non-cardiac arrest call. CAB, on the other hand, is now being used during cardiac arrest to remind practitioners and laypeople of the importance of compressions. In general, it is not useful to confine yourself to one ideology "because they say so." It is much more productive to understand each approach and use critical thinking to choose the best route for your patient.
That's all
-Upasana Y. :)
Saucerization and Arthrodesis
I was fascinated with this two terms :- Saucerization in Osteomyelitis and Arthrodesis (I studied it in treatment of foot drop).
SAUCERIZATION
-Extension of surgical debridement
-Debrided wounds left open widely through excision of overhanging soft tissue and bone
-Wounds drain freely (otherwise If we close it the pus will keep on collecting)
-Abscesses do not form
-Limited to areas where it causes acceptable loss of function e.g. Tibia and femur
Arthrodesis
The term arthrodesis refers to surgical fusion of a joint.
The indications for this are pain & instability in a joint and, in some situations, following the failure of joint replacement.
FIXATION POSITIONS
The optimum positions for arthrodesis in different joints are as follows:
1. SHOULDER:
-In such a position that the hand can comfortably reach the mouth.
-The person will be able to perform the day-to-day activity like eating.combing,scratching the back,cleaning.
-Arthrodesis of shoulder joint is usually reserved for a flail joint as may follow a brachial plexus injury.
-Stabilization of this joint may lead to improvement in the remaining distal function of the arm.
2. ELBOW: 90° of flexion.
(Suppose you won't be able to flex it 90 degree ,then what will happen? Try eating food with that position. You won't be able to do that without this.)
3. WRIST: A few degree of extension
4. THUMB:
-MCP joint in 20° of flexion.
-IP joint in slight flexion.
5.FINGERS:
MCP joints in 20° -30° of flexion.
(These joints are rarely fused).
Proximal IP joints in 40° -45° of flexion (less in middle & index fingers)

Casts (Colle's Cast)
These days, I am attending orthopaedics posting. And I am loving it.
I saw casting. Following questions were asked to me during the procedure.
Q. Define Casts and Slabs.
A. Cast & slab are methods of a temporary immobilization for a wide variety of musculoskeletal conditions not only for disorders of bones but also for many other disorders related with tendons, muscles and soft tissues
Cast: are circumferential immobilizers which is surrounding the whole circumference of the limb
Slab: are non-circumferential immobilizers which is only support apart of the circumference of the limb.
Q. Define Traction and Splints.
A. TRACTION -Traction is a method of restoring alignment to a fracture through gradual neutralisation of muscular forces. Traction is applied to the limb distal to the fracture, so as to exert a continuous pull in the long axis of the bone.
SPLINT - A device used for support or immobilization of a limb or the spine. Any material used to support a fracture is known as splint.
Q. What is Colle's Fracture?
A. It is not just fracture lower end of radius but a fracture dislocation of the inferior radioulnar joint.
Q. Do you know anything regarding Colles Cast.
A. It is a type of Immobilization method. It is the Below elbow cast (10 – 20 degree palmar flexion, 15 – 20 degree ulnar deviation) .
So, Colle`s cast :- It is a below elbow cast in supination.
Ideally it has to meet the following 4 criteria :
-Firm fit at the dorsum
-Firm fit at the volar fracture apex
-Just snuggly fitting at the forearm
-Metacarpophalangeal joints should be free to move.
Arsenic Poisoning
Hello awesomites!
Here's a Mnemonic on Arsenic Poisoning
The mnemonic is AR4SENIC
A-Aldrich Mees line (Nail)
R-Raindrop pigmentation
Reinsch Test (Gutzeit test used nowadays)
Rashes(fading measles rashes)
Red velvety mucosa(Postmortem finding)
S-Subendocardial hemorrhage(Postmortem finding)
E-Excess pigmentation and keratosis (Palms and soles)
N-Neuritis
I-Iron oxide n BAL(antidote)
C-Cholera like symptoms
I hope that it's helpful.
That's all!
Thank you.
Diagnostic criteria of neurofibromatosis type 1 mnemonic
The criteria are met in an individual if two or more of the features listed are present.
The mnemonic is "FANCOOL"
F: Family history
A: Axillary freckles (known as CROWE'S SIGN)
N: Neurofibromas (2 or more)
C: Café-au-lait macules (6 or more)
O: Optic gliomas
O: Osseous (sphenoid dysplasia)
L: Lisch nodules in the eyes.
Thanks for reading.
Madhuri
Sunday, August 13, 2017
Diagnostic features in the X-ray and probable pathology in the Sinus
1. Haziness of sinuses only :- Sinusitis
2. Bony expansion without erosion :- Benign tumefaction e.g Polyposis
3. Decreased air shadow in nasal cavity without bony expansion :- Hypertrophic rhinitis
4. Bony erosion with expansion :- Malignancy
5. Bony defect without expansion of haziness :- Surgically induced (Iatrogenic) or fracture
6. Fluid level in maxillary sinus :- Sinusitis with pus signifying acute bacterial maxillary sinusitis
This question was asked to me by my friend and it was fun to find the answer.
(Source :-Otolaryngology at the eleventh hour By Anupam Mishra)
That's all for today.
-Upasana Y. :)
Saturday, August 12, 2017
New treatment regimen for Hepatitis C
Hey guys! I have copied this article from the FDA website more or less. You will definitely find it helpful.
The U.S. Food and Drug Administration today approved Mavyret (glecaprevir and pibrentasvir) to treat adults with chronic hepatitis C virus (HCV) genotypes 1-6 without cirrhosis (liver disease) or with mild cirrhosis, including patients with moderate to severe kidney disease and those who are on dialysis. Mavyret is also approved for adult patients with HCV genotype 1 infection who have been previously treated with a regimen either containing an NS5A inhibitor or an NS3/4A protease inhibitor but not both.
Mavyret is the first treatment of eight weeks duration approved for all HCV genotypes 1-6 in adult patients without cirrhosis who have not been previously treated. Standard treatment length was previously 12 weeks or more.
“This approval provides a shorter treatment duration for many patients, and also a treatment option for certain patients with genotype 1 infection, the most common HCV genotype in the United States, who were not successfully treated with other direct-acting antiviral treatments in the past,” said Edward Cox, M.D., director of the Office of Antimicrobial Products in the FDA’s Center for Drug Evaluation and Research.
There are at least six distinct HCV genotypes, or strains, which are genetically distinct groups of the virus. Knowing the strain of the virus can help inform treatment recommendations.
The safety and efficacy of Mavyret were evaluated during clinical trials enrolling approximately 2,300 adults with genotype 1, 2, 3, 4, 5 or 6 HCV infection without cirrhosis or with mild cirrhosis. Results of the trials demonstrated that 92-100 percent of patients who received Mavyret for eight, 12 or 16 weeks duration had no virus detected in the blood 12 weeks after finishing treatment, suggesting that patients’ infection had been cured.
Treatment duration with Mavyret differs depending on treatment history, viral genotype, and cirrhosis status.
The most common adverse reactions in patients taking Mavyret were headache, fatigue and nausea.
Mavyret is not recommended in patients with moderate cirrhosis and contraindicated in patients with severe cirrhosis. It is also contraindicated in patients taking the drugs atazanavir and rifampin.
That's all!
-VM
Thursday, August 10, 2017
Factors increasing iron absorption in the intestine mnemonic
Did you know a number of dietary factors influence iron absorption?
Ascorbate (vitamin C) and citrate increase iron uptake in part by acting as weak chelators to help solubilize it in the duodenum.
Cushing Ulcers : An overview
Hi Everyone ! Here's a short post on Cushing and Curling ulcers.
For Cushing Ulcers you need to remember these key points :
C
U - Ulcerating - can even perforate.
S - Stomach
H - Head injury induced Stress Ulcer
I - lNcreased
N - INcreased
G - Gastric Acid secretion.
Stress ulcers are typically non ulcerative superficial erosions of the gastric mucosa.
They occur when a person is subjected to physical stress in the form of Trauma, Sepsis, Burns, Hemorrhage among many others.
Psychological stress doesn't cause 'Stress ulcers' , although it does pre dispose to getting Peptic Ulcer Disease on its own accord. All the same, it doesn't cause 'Stress ulcer'.
Cushing ulcers are type of stress ulcers occuring secondary to Head injury. They occur in the stomach commonly , and are associated with increased Gastric acid secretion. They are typically erosive and ulcerative , more likely to perforate than other stress ulcers.
Another named stress ulcer is Curling Ulcer occuring secondary to Burns. They occur in the 1st part of duodenum commonly , and are NOT associated with increased Gastric acid secretion.
Presentation :
Painless upper GI bleeding within 1-2 days of traumatic event.
Usually slow and intermittent bleeding.
Diagnosis :
Endoscopy.
(More to rule out other causes of GI bleed rather than ruling this in).
Treatment :
- Treat underlying causes.
- Fluids
- Gastric pH to be maintained > 5 (using PPI like Pantoprazole)
- If lot of bleeding - Ligation of vessel at base of ulcer.
That's all!
Happy studying !
Stay awesome !
~ A.P.Burkholderia
Image Based MCQ on Ophthalmology
Yesterday we posted an Image based MCQ on Ophthalmology and here is the answer for it.
#Ophthalmology
#Spot_Dx
Q. What is the most likely diagnosis of the given image?

B. Symblepharon
C. Pterygium
D. Pseudo pterygium
The correct answer is B. Symblepharon.
Symblepharon is an adhesion between the eyelid and the eyeball. It can involve just one lid or both. This adhesion of subepithelial scarring can lead to other lid complications such as aberrant lash growth and entropion. Symblepharon can develop as a complication of several diseases and/or etiologies that include:
Severe dry eye syndrome
Stevens-Johnson syndrome
Cicatricial pemphigoid
Chemical injury
Erythema multiforme
Bullous pemphigus
Conjunctival infections associated with conjunctival scarring such as chlamydial, vernal, atopic, and bacterial conjunctivitis
Epidemic keratoconjunctivitis
Burns
Toxic epidermal necrosis
Thank you.
Tuesday, August 8, 2017
Pulmonary Alveolar Proteinosis: High yield points
Pulmonary Alveolar Proteinosis (PAP)
a. Lipoproteinaceous material(like surfactant) accumulates within alveoli.
b. There is susceptibility to pulmonary infections, sometimes with opportunistic organisms.
c. In the congenital form, there is mutation in the gene for surfactant protein B or C or the Bc chain of the receptor for GM-CSF.
d. It can be secondary to Hematologic cancers, pharmacologic immunosuppression, inhalation of organic dust (eg., silica) or toxic fumes and certain infections.
e. Acquired PAP is an autoimmune disease targeting GM-CSF.
f. 72 percent patients have a history of smoking.
g. Most patients present with progressive exertional dyspnea of insidious onset and cough. If there is secondary infection, there can also be fever, chest pain, hemoptysis.
h. Physical examination: Some patients have cyanosis, clubbing, inspiratory crackles.
i. Chest X ray: Bilateral air-space disease with an ill-defined nodular or confluent pattern.
j. HRCT: Patchy, ground glass opacifications with superimposed interlobular septal and intralobular thickening, a pattern called "Crazy Paving".
k. The lavage fluid in patients with this disorder has an opaque, milky appearance. It is PAS positive.
l. Electron Microscopy shows that the intraalveolar material consists of amorphous, granular debris containing numerous osmiophilic, fused membrane structures resembling lamellar bodies and tubular myelin.
m. Acquired PAP has been treated successfully by Whole-lung lavage.
-VM
Myopathies series - Part 7
In previous post, We discussed about myopathy caused due to structural changes.
Today, I will explain it in detail. (SOURCE :- Harrison's Principle of internal medicine )
Two complex are important here :-
1. DYSTROPHIN COMPLEX
2. SARCOGLYCAN COMPLEX
- Dystrophin-glycoprotein complex confer stability to the sarcolemma
- deficiency of dystrophin (Duchennes dystrophy) may lead to secondary loss of the sarcoglycans and dystroglycan
-Loss of a single sarcoglycan (LGMD) results in secondary loss of other sarcoglycans in the membrane without affecting dystrophin
-Disruption of the dystrophin-glycoprotein complexes weakens the sarcolemma, causing membrane tears and a cascade of events leading to muscle fiber necrosis.
Let us discuss dystrophinopathies first .
1.Duchene’s muscular dystrophy
-Most common muscular dystrophy
- X-linked recessive disorder
- Onset before age 5
-Age : Present at birth ,Usually becomes apparent between ages 3 and 5
-Sex : Male
Etiology
-XR (Deletion mutation of the gene that encodes dystrophin)
Laboratory Tests
• Serum CK
– Elevated to between 20 and 100 times normal
– Abnormal at birth but declines late in the disease because of inactivity and loss of muscle mass.
Mutation analysis on peripheral blood leukocytes
• Identification of a specific mutation in dystrophin gene
– Allows for unequivocal diagnosis
– Makes possible accurate testing of potential carriers
– Is useful for prenatal diagnosis
Diagnostic Procedures
• EMG -> Myopathic
Muscle biopsy
• Muscle fibers of varying size
• Small groups of necrotic and regenerating fibers
• Connective tissue and fat replace lost muscle fibers.
• Definitive diagnosis is established on the basis of dystrophin deficiency.
• Diagnosis can also be made by Western blot analysis of muscle biopsy specimens.
– Abnormalities on the quantity and molecular weight of dystrophin protein
• Immunocytochemical staining of muscle with dystrophin antibodies
– Can be used to demonstrate absence or deficiency of dystrophin
– localizing to the sarcolemmal membrane
– Possible mosaic pattern in carriers of the disease
– Dystrophin analysis of muscle biopsy specimens for carrier detection not reliable
Treatments
Prednisone 0.75 mg/kg per d
– Significantly slows progression for up to 3 years
– Some patients cannot tolerate glucocorticoid therapy
• Weight gain is significant
– Complications of long-term use often outweigh the benefits.
Exon skipping therapy
• Duchenne's disease may benefit from novel therapies that either replace the defective gene or missing protein or implement downstream corrections (e.g., skipping mutated exons or reading through mutations that introduce stop codons)
2. Becker’s Muscular dystrophy
-Less-severe form of XR muscular dystrophy
-allelic defects of same gene of Duchenne ( ~10 times less frequent than Duchenne)
-Age : – Most between ages 5 and 15
– Onset in the third or fourth decade or even later can occur
- Sex : Male
Symptoms & Signs
• Onset of symptoms occurs between ages 5 and 15.
I.Muscular manifestations – Pattern of muscle wasting closely resembles Duchenne.
– Progressive weakness of girdle muscles, especially of lower extremities
– Weakness becomes generalized as disease progresses.
– Hypertrophy, particularly in calves, is an early and prominent finding.
– By definition, patients walk beyond age 15 (whereas patients with Duchenne dystrophy are typically in a wheelchair by the age of 12).
– Significant facial muscle weakness is not a feature.
– Respiratory failure may develop by fourth decade.
II. Extramuscular manifestations
– Cardiac, may result in heart failure
– Mental retardation may occur, not as common as in Duchenne
• Other less common presentations
– Asymptomatic hyper-CK-emia
– Myalgias without weakness
– Myoglobinuria
Laboratory Tests
• Serum CK – Closely resembles findings in Duchenne dystrophy
• Mutation analysis on peripheral blood leukocytes
– Deletions or duplications of the dystrophin gene in 65% of patients (same as in Duchennes dystrophy)
– 95% of patients, the DNA deletion does not alter the translational reading frame of mRNA.
These "in-frame" mutations allow for production of some dystrophin, which accounts for the presence of altered rather than absent dystrophin on Western blot analysis
• EMG – Myopathic
• Muscle biopsy – Results closely resemble those in Duchenne dystrophy.
– Diagnosis requires Western blot analysis of muscle biopsy samples demonstrating a reduced amount or abnormal size of dystrophin.
Treatments
• Use of glucocorticoids has not been adequately studied
• Endurance training may be helpful

That's all for today.
-Upasana Y. :)
Composition of Bone cement
Today I saw a case of Infected AMP implant. Following questions were asked to me regarding bone cement.
Q. Composition of bone cement.
A. Bone cement consist of :- Powder and liquid.
POWDER
1. Polymer : Polymethylmethacrylate (PMMA)
2. Initiator : Benzoyl peroxide (BPO)
3. Radio-opacifier : Barium sulphate , Zirconia
4. Antibiotic :- Gentamicin (commonly)
LIQUID
1. Monomer : Methylmethacrylate (MMA)
2. Accelerator : N,N Dimethy Paratoluidine (DMPT)
3. Stabilizer : Hydroquinone
Q.Antibiotics used as additives for PMMA bone cement.
A. Antibiotics commonly used as additives for PMMA bone cement include:
- vancomycin, (MRSA)
-gentamicin,
-meropenem,
-in addition to tobramycin.
Also, successful non-antibiotic bactericides that have been used as bone cement additives include:-
- Quaternary ammonium compounds (benzalkonium chloride and cetylpyridinium chloride)
That's all for today.
-Upasana Y. :)
Monday, August 7, 2017
Causes of Radio Radial and Radio femoral delay
Before this post I didn't realise the importance of checking and comparing both the radial pulses.
Pulse, by definition, is the expansion and elongation of the arterial wall imparted by the column of blood, passively produced by the pressure changes during ventricular systole and diastole.
Always report the pulse under following headings.
Assessment of pulse include :-
1. RATE (beats/min)
-Tachycardia (>100bpm)
-bradycardia (<60bpm)
2.RHYTHM
-regular
-regularly irregular (2nd degree heart block)
-Irregularly irregular (Atrial fibrillation, ventricular premature beat)
3.EQUALITY
4.CHARACTER
5.PERIPHERAL PULSES
6.APEX PULSE DEFICIT (atrial fibrillation )
7. RADIO RADIAL /RADIO FEMORAL DELAY
Today , I will discuss the causes of Radio Radial and Radio Femoral delay.
CAUSES OF RADIO RADIAL DELAY :-
1. Normal anatomical variations
2. Thoracic inlet syndrome, e.g. cervical rib
3. Aneurysm of Arch of aorta
4. Presubclavian coarctation
5. Supravalvular aortic stenosis
6. Pulseless disease
7. Peripheral embolism or artheromatous plaques
8. Artherosclerosis of aorta
9. Pressure over axillary artery by lymph nodes
10. Iatrogenic, Blalock-Tausig shunt operation in TOF
CAUSES OF RADIO FEMORAL DELAY :-
1. Coarctation of aorta
2. Artherosclerosis of aorta
3. Thrombosis or embolism of aorta
4. Aortoarteritis
That's all for today,
-Upasana Y. :)
Iodized salt test
We all know that salt is used as a medium for iodization.
Iodized salt is used prophylactically to prevent endemic goiter as public health importance.
Iodide deficiency disorder IDD include :-
-goiter
-Hypothyroidism
- Subnormal intelligence
-Mental retardation
-Neuromuscular weakness
-Hearing and speech defect
-endemic cretinism
-Still birth
To check whether given packet of salt contain iodine or not, we use different method.
Rapid kit test is one of the test.
The kit consist of 2 ampoule test solution and 1 recheck solution bottle.
In the diagram I made 3 bottles to represent the 3 component of the test.
Alkalinity of salt doesn't give colour. So we use recheck solution in the end of the test .
The colour of the test sample is compared with the standard colour chart for calculating the salt iodine content.


Microbiology question

#Microbiology
#Medicowesome
A patient is suffering from features of septic shock with following clinical picture.Most probable causative organism is
A) Staphylococcus
B) Listeria
C) CMV
D) Meningococcus
It is a classical case of Waterhouse-friderichsen syndrome/Purpura fulminans/Fulminant meningococcemia:It is simply trauma to adrenal gland causing extensive bleeding, multiple organ failure, leucopenia, thromobocytopenia and consistent development of DIC.Low level of blood glucose and sodium and high level of ACTH and potassium level is suggestive of adrenal failure.
It differs from other septic shock because of the presence of prominent hemorrhagic skin lesions petechia, purpura.
Sunday, August 6, 2017
Image Based MCQ on Twin Pregnancy
#Obs_Gynae
Q. What is the diagnosis of the given USG image?

Saturday, August 5, 2017
Hill’s criteria in Aortic Regurgitation
Mild - difference of 20-40 mmHg
Moderate - difference of 40-60 mmHg
Severe - difference of >60 mmHg.
Hope that helped :)
- Jaskunwar Singh
Image based MCQ on pediatric infections
Yesterday we posted an MCQ on a pediatric infection with characteristic appearance of rash on face, involving both cheeks.
Friday, August 4, 2017
Image Based MCQ on Fracture
Yesterday we posted an Image based MCQ on Fracture of forearm bones and here's the answer for it.
Q. The X-ray of forearm in AP and Lateral views as shown in the image is diagnostic of

B. Barton fracture
C. Monteggia fracture-dislocation
D. Colles fracture
Type II: posterior dislocation of radial head
Type III: lateral dislocation of radial head
Type IV: anterior radial head dislocation as well as proximal third ulnar and radial shaft fractures
Thanks for your active participation.
Thursday, August 3, 2017
Causes of chemosis mnemonic
Chemosis is known as oedema of conjunctiva.
Reason:due to exudation from the abnormal capillaries.This retained exudate gives a swollen and gelatinous appearance.
Regions: loosely attached areas of the bulbar conjunctiva and fornices.
Causes: ABC
A: Acute inflammations like gonococcal conjunctivitis, panophthalmitis, dacryocystitis, periostitis, orbital cellulitis.
B: Blood conditions (abnormal) like anaemia, urticaria, angioneurotic oedema, lymphocytic infiltration.
C: Circulatory obstruction in conditions like pulsating exophthalmos or due to pressure of an orbital tumour which may interfere with the lymph and blood drainage.
Thanks for reading.
Madhuri
Causes of hematuria mnemonic
( mnemonic: GH )
- Glomerulonephritis ( post infectious, membranoproliferative, rapid progressive, IgA nephropathy )
- Henoch- Schonlein nephritis
( mnemonic : HEMATURIa )
- Hemorrhage ( cystitis, PCKD )
- Allergic reaction ( interstitial nephritis )
- Trauma or Tumors
- Urinary tract infections / increased Urinary calcium
Renal colic : Important points
Wednesday, August 2, 2017
Tay Sachs Disease
Hello Awesomites!
Here's a Blog on Tay Sachs Disease and some common questions related to it.
Tay-Sachs disease
It is a genetic disorder that results in the destruction of nerve cells in the brain and spinal cord. Tay–Sachs disease is caused by a genetic mutation in the HEXA genes on chromosome 15. It is inherited from a person's parents in an autosomal recessive manner. The mutation results in problems with an enzyme called beta-hexosamidase A ,located on lysosomes,which results in the build up of the toxin GM2 ganglioside within cells. The most common type, known as infantile Tay–Sachs disease, becomes apparent around three to six months of age with the baby losing the ability to turn over, sit, or crawl. This is then followed by seizures, hearing loss, and inability to move. An eye abnormality called a cherry-red spot, which can be identified with an eye examination, is characteristic of this disorder. Death usually occurs in early childhood. Less commonly the disease may occur in later childhood or adulthood. These forms are generally milder in nature.Diagnosis is by measuring the blood hexosaminidase A level or genetic testing.
Frequently asked questions -
The substance which accumulates in Tay Sach’s disease is Ganglioside.
Deficiency of enzyme Hexosaminidase-A causes Tay Sach’s disease.
Cherry red spot at macula may be seen in Tay Sach’s disease.
That's all!
Thank you.
MD Mobarak Hussain (Maahii)
Myopathies series - Part 6
Now we will discuss individual myopathies in detail.

We have discussed the association between metabolic disorder and myopathies.
Metabolic myopathies Intro
Metabolic myopathies (differential diagnosis)
In this part, we will discuss the association between structure of cell (myocytes) and myopathy. Look at the diagrams below :-







I hope it helped.
-Upasana Y. :)